Related Research Articles

Pancreatitis is a condition characterized by inflammation of the pancreas. The pancreas is a large organ behind the stomach that produces digestive enzymes and a number of hormones. There are two main types: acute pancreatitis, and chronic pancreatitis.

Respiratory failure results from inadequate gas exchange by the respiratory system, meaning that the arterial oxygen, carbon dioxide, or both cannot be kept at normal levels. A drop in the oxygen carried in the blood is known as hypoxemia; a rise in arterial carbon dioxide levels is called hypercapnia. Respiratory failure is classified as either Type 1 or Type 2, based on whether there is a high carbon dioxide level, and can be acute or chronic. In clinical trials, the definition of respiratory failure usually includes increased respiratory rate, abnormal blood gases, and evidence of increased work of breathing. Respiratory failure causes an altered mental status due to ischemia in the brain.

Mechanical ventilation or assisted ventilation is the medical term for using a machine called a ventilator to fully or partially provide artificial ventilation. Mechanical ventilation helps move air into and out of the lungs, with the main goal of helping the delivery of oxygen and removal of carbon dioxide. Mechanical ventilation is used for many reasons, including to protect the airway due to mechanical or neurologic cause, to ensure adequate oxygenation, or to remove excess carbon dioxide from the lungs. Various healthcare providers are involved with the use of mechanical ventilation and people who require ventilators are typically monitored in an intensive care unit.

Tidal volume is the volume of air moved into or out of the lungs in one breath. In a healthy, young human adult, tidal volume is approximately 500 ml per inspiration at rest or 7 ml/kg of body mass.

Extracorporeal membrane oxygenation (ECMO), is a form of extracorporeal life support, providing prolonged cardiac and respiratory support to persons whose heart and lungs are unable to provide an adequate amount of oxygen, gas exchange or blood supply (perfusion) to sustain life. The technology for ECMO is largely derived from cardiopulmonary bypass, which provides shorter-term support with arrested native circulation. The device used is a membrane oxygenator, also known as an artificial lung.

Acute respiratory distress syndrome (ARDS) is a type of respiratory failure characterized by rapid onset of widespread inflammation in the lungs. Symptoms include shortness of breath (dyspnea), rapid breathing (tachypnea), and bluish skin coloration (cyanosis). For those who survive, a decreased quality of life is common.

Epiglottitis is the inflammation of the epiglottis—the flap at the base of the tongue that prevents food entering the trachea (windpipe). Symptoms are usually rapid in onset and include trouble swallowing which can result in drooling, changes to the voice, fever, and an increased breathing rate. As the epiglottis is in the upper airway, swelling can interfere with breathing. People may lean forward in an effort to open the airway. As the condition worsens, stridor and bluish skin may occur.

Non-invasive ventilation (NIV) is the use of breathing support administered through a face mask, nasal mask, or a helmet. Air, usually with added oxygen, is given through the mask under positive pressure; generally the amount of pressure is alternated depending on whether someone is breathing in or out. It is termed "non-invasive" because it is delivered with a mask that is tightly fitted to the face or around the head, but without a need for tracheal intubation. While there are similarities with regard to the interface, NIV is not the same as continuous positive airway pressure (CPAP), which applies a single level of positive airway pressure throughout the whole respiratory cycle; CPAP does not deliver ventilation but is occasionally used in conditions also treated with NIV.
Necrotizing enterocolitis (NEC) is a devastating intestinal disease that affects premature or very low birth weight infants. Symptoms may include poor feeding, bloating, decreased activity, blood in the stool, vomiting of bile, multi-organ failure, and even death.
Tracheobronchitis is inflammation of the trachea and bronchi. It is characterised by a cough, fever, and purulent sputum and is therefore suggestive of pneumonia. It is classified as a respiratory tract infection.
Ventilator-associated pneumonia (VAP) is a type of lung infection that occurs in people who are on mechanical ventilation breathing machines in hospitals. As such, VAP typically affects critically ill persons that are in an intensive care unit (ICU) and have been on a mechanical ventilator for at least 48 hours. VAP is a major source of increased illness and death. Persons with VAP have increased lengths of ICU hospitalization and have up to a 20–30% death rate. The diagnosis of VAP varies among hospitals and providers but usually requires a new infiltrate on chest x-ray plus two or more other factors. These factors include temperatures of >38 °C or <36 °C, a white blood cell count of >12 × 109/ml, purulent secretions from the airways in the lung, and/or reduction in gas exchange.

Respiratory tract infections (RTIs) are infectious diseases involving the lower or upper respiratory tract. An infection of this type usually is further classified as an upper respiratory tract infection or a lower respiratory tract infection. Lower respiratory infections, such as pneumonia, tend to be far more severe than upper respiratory infections, such as the common cold.
Positive end-expiratory pressure (PEEP) is the pressure in the lungs above atmospheric pressure that exists at the end of expiration. The two types of PEEP are extrinsic PEEP and intrinsic PEEP. Pressure that is applied or increased during an inspiration is termed pressure support.PEEP is a therapeutic parameter set in the ventilator, or a complication of mechanical ventilation with air trapping (auto-PEEP).
High-frequency ventilation is a type of mechanical ventilation which utilizes a respiratory rate greater than four times the normal value and very small tidal volumes. High frequency ventilation is thought to reduce ventilator-associated lung injury (VALI), especially in the context of ARDS and acute lung injury. This is commonly referred to as lung protective ventilation. There are different types of high-frequency ventilation. Each type has its own unique advantages and disadvantages. The types of HFV are characterized by the delivery system and the type of exhalation phase.
Ventilator-associated lung injury (VALI) is an acute lung injury that develops during mechanical ventilation and is termed ventilator-induced lung injury (VILI) if it can be proven that the mechanical ventilation caused the acute lung injury. In contrast, ventilator-associated lung injury (VALI) exists if the cause cannot be proven. VALI is the appropriate term in most situations because it is virtually impossible to prove what actually caused the lung injury in the hospital.

Airway pressure release ventilation (APRV) is a pressure control mode of mechanical ventilation that utilizes an inverse ratio ventilation strategy. APRV is an applied continuous positive airway pressure (CPAP) that at a set timed interval releases the applied pressure. Depending on the ventilator manufacturer, it may be referred to as BiVent. This is just as appropriate to use, since the only difference is that the term APRV is copyrighted.
Pneumonia can be classified in several ways, most commonly by where it was acquired, but may also by the area of lung affected or by the causative organism. There is also a combined clinical classification, which combines factors such as age, risk factors for certain microorganisms, the presence of underlying lung disease or systemic disease and whether the person has recently been hospitalized.
Modes of mechanical ventilation are one of the most important aspects of the usage of mechanical ventilation. The mode refers to the method of inspiratory support. In general, mode selection is based on clinician familiarity and institutional preferences, since there is a paucity of evidence indicating that the mode affects clinical outcome. The most frequently used forms of volume-limited mechanical ventilation are intermittent mandatory ventilation (IMV) and continuous mandatory ventilation (CMV). There have been substantial changes in the nomenclature of mechanical ventilation over the years, but more recently it has become standardized by many respirology and pulmonology groups. Writing a mode is most proper in all capital letters with a dash between the control variable and the strategy.
Prone ventilation, sometimes called prone positioning or proning, is a method of mechanical ventilation with the patient lying face-down (prone). It improves oxygenation in most patients with acute respiratory distress syndrome (ARDS) and reduces mortality. The earliest trial investigating the benefits of prone ventilation occurred in 1976. Since that time, many meta-analyses and one randomized control trial, the PROSEVA trial, have shown an increase in patients' survival with the more severe versions of ARDS. There are many proposed mechanisms, but they are not fully delineated. The proposed utility of prone ventilation is that this position will improve lung mechanics, improve oxygenation, and increase survival. Although improved oxygenation has been shown in multiple studies, this position change's survival benefit is not as clear. Similar to the slow adoption of low tidal volume ventilation utilized in ARDS, many believe that the investigation into the benefits of prone ventilation will likely be ongoing in the future.
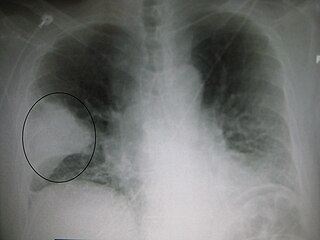
Necrotizing pneumonia (NP), also known as cavitary pneumonia or cavitatory necrosis, is a rare but severe complication of lung parenchymal infection. In necrotizing pneumonia, there is a substantial liquefaction following death of the lung tissue, which may lead to gangrene formation in the lung. In most cases patients with NP have fever, cough and bad breath, and those with more indolent infections have weight loss. Often patients clinically present with acute respiratory failure. The most common pathogens responsible for NP are Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae. Diagnosis is usually done by chest imaging, e.g. chest X-ray, CT scan. Among these CT scan is the most sensitive test which shows loss of lung architecture and multiple small thin walled cavities. Often cultures from bronchoalveolar lavage and blood may be done for identification of the causative organism(s). It is primarily managed by supportive care along with appropriate antibiotics. However, if patient develops severe complications like sepsis or fails to medical therapy, surgical resection is a reasonable option for saving life.
References
- ↑ Wilson, Kent S.; Carley, Richard B.; Ophoven, Janice P.; Mammel, Mark C.; Boros, Stephen J. (1987). "Necrotizing tracheobronchitis: A newly recognized cause of acute obstruction in mechanically ventilated neonates". The Laryngoscope. 97 (9): 1017–9. doi: 10.1288/00005537-198709000-00003 . PMID 3626723.
- ↑ Chechani, V; Vasudevan, V. P.; Kamholz, S. L. (1991). "Necrotizing tracheobronchitis: Complication of mechanical ventilation in an adult". Southern Medical Journal. 84 (2): 271–3. doi:10.1097/00007611-199102000-00031. PMID 1990468.
| | This article about a medical condition affecting the respiratory system is a stub. You can help Wikipedia by expanding it. |