Related Research Articles

The outer ear, external ear, or auris externa is the external part of the ear, which consists of the auricle and the ear canal. It gathers sound energy and focuses it on the eardrum.
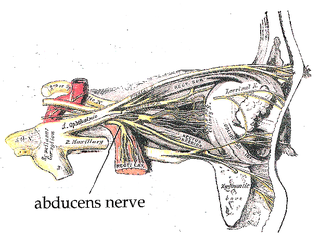
The abducens nerve or abducent nerve, also known as the sixth cranial nerve, cranial nerve VI, or simply CN VI, is a cranial nerve in humans and various other animals that controls the movement of the lateral rectus muscle, one of the extraocular muscles responsible for outward gaze. It is a somatic efferent nerve.

The facial nerve, also known as the seventh cranial nerve, cranial nerve VII, or simply CN VII, is a cranial nerve that emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerve typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises from the brainstem from an area posterior to the cranial nerve VI and anterior to cranial nerve VIII.
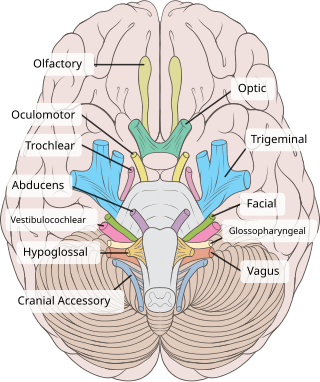
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
The trochlear nerve, also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye. Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve.
The glossopharyngeal nerve, also known as the ninth cranial nerve, cranial nerve IX, or simply CN IX, is a cranial nerve that exits the brainstem from the sides of the upper medulla, just anterior to the vagus nerve. Being a mixed nerve (sensorimotor), it carries afferent sensory and efferent motor information. The motor division of the glossopharyngeal nerve is derived from the basal plate of the embryonic medulla oblongata, whereas the sensory division originates from the cranial neural crest.

The vestibulo-ocular reflex (VOR) is a reflex acting to stabilize gaze during head movement, with eye movement due to activation of the vestibular system. The reflex acts to stabilize images on the retinas of the eye during head movement. Gaze is held steadily on a location by producing eye movements in the direction opposite that of head movement. For example, when the head moves to the right, the eyes move to the left, meaning the image a person sees stays the same even though the head has turned. Since slight head movement is present all the time, VOR is necessary for stabilizing vision: people with an impaired reflex find it difficult to read using print, because the eyes do not stabilise during small head tremors, and also because damage to reflex can cause nystagmus.
Otoplasty denotes the surgical and non-surgical procedures for correcting the deformities and defects of the pinna, and for reconstructing a defective, or deformed, or absent external ear, consequent to congenital conditions and trauma. The otoplastic surgeon corrects the defect or deformity by creating an external ear that is of natural proportions, contour, and appearance, usually achieved by the reshaping, the moving, and the augmenting of the cartilaginous support framework of the pinna. Moreover, the occurrence of congenital ear deformities occasionally overlaps with other medical conditions.

Friedrich Wilhelm Ernst Albrecht von Gräfe, often Anglicized to Graefe, was a Prussian pioneer of German ophthalmology. Graefe was born in Finkenheerd, Brandenburg, the son of Karl Ferdinand von Graefe (1787–1840). He was the father of the far right politician Albrecht von Graefe (1868–1933).

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.

The lateral rectus muscle is a muscle on the lateral side of the eye in the orbit. It is one of six extraocular muscles that control the movements of the eye. The lateral rectus muscle is responsible for lateral movement of the eyeball, specifically abduction. Abduction describes the movement of the eye away from the midline, allowing the eyeball to move horizontally in the lateral direction, bringing the pupil away from the midline of the body.

The abducens nucleus is the originating nucleus from which the abducens nerve (VI) emerges—a cranial nerve nucleus. This nucleus is located beneath the fourth ventricle in the caudal portion of the pons near the midline, medial to the sulcus limitans.
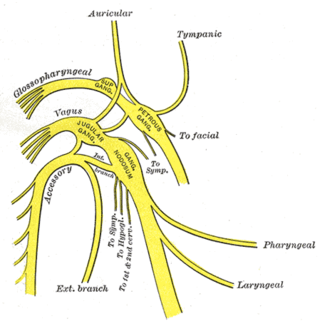
The auricular branch of the vagus nerve is often termed the Alderman's nerve or Arnold's nerve. The latter name is an eponym for Friedrich Arnold. The auricular branch of the vagus nerve supplies sensory innervation to the skin of the ear canal, tragus, and auricle.
Sixth nerve palsy, or abducens nerve palsy, is a disorder associated with dysfunction of cranial nerve VI, which is responsible for causing contraction of the lateral rectus muscle to abduct the eye. The inability of an eye to turn outward, results in a convergent strabismus or esotropia of which the primary symptom is diplopia in which the two images appear side-by-side. Thus, the diplopia is horizontal and worse in the distance. Diplopia is also increased on looking to the affected side and is partly caused by overaction of the medial rectus on the unaffected side as it tries to provide the extra innervation to the affected lateral rectus. These two muscles are synergists or "yoke muscles" as both attempt to move the eye over to the left or right. The condition is commonly unilateral but can also occur bilaterally.
The superior ganglion of the vagus nerve, (jugular ganglion) is a sensory ganglion of the peripheral nervous system. It is located within the jugular foramen, where the vagus nerve exits the skull. It is smaller than and proximal to the inferior ganglion of the vagus nerve.

Marcus Gunn phenomenon is an autosomal dominant condition with incomplete penetrance, in which nursing infants will have rhythmic upward jerking of their upper eyelid. This condition is characterized as a synkinesis: when two or more muscles that are independently innervated have either simultaneous or coordinated movements.
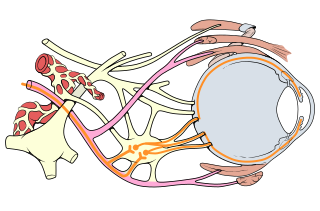
Oculomotor nerve palsy or oculomotor neuropathy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Damage to this nerve will result in an inability to move the eye normally. The nerve also supplies the upper eyelid muscle and is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movement resulting from the condition are generally so severe that patients are often unable to maintain normal eye alignment when gazing straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).
Chronic progressive external ophthalmoplegia (CPEO) is a type of eye disorder characterized by slowly progressive inability to move the eyes and eyebrows. It is often the only feature of mitochondrial disease, in which case the term CPEO may be given as the diagnosis. In other people suffering from mitochondrial disease, CPEO occurs as part of a syndrome involving more than one part of the body, such as Kearns–Sayre syndrome. Occasionally CPEO may be caused by conditions other than mitochondrial diseases.

The posterior auricular muscle is a muscle behind the auricle of the outer ear. It arises from the mastoid part of the temporal bone, and inserts into the lower part of the cranial surface of the auricle of the outer ear. It draws the auricle backwards, usually a very slight effect.
The Lazarus sign or Lazarus reflex is a reflex movement in brain-dead or brainstem failure patients, which causes them to briefly raise their arms and drop them crossed on their chests. The phenomenon is named after the Biblical figure Lazarus of Bethany, whom Jesus raised from the dead according to the Gospel of John.
References
- ↑ Caplan, Louis R.; Hopf, Hanns C. (2012-12-06). Brain-Stem Localization and Function. Springer Science & Business Media. ISBN 9783642781728.
- ↑ Schmidt, D.; Thoden, U. (1978-06-19). "Co-activation of the M. transversus auris with eye movements (Wilson's oculo-auricular phenomenon) and with activity in other cranial nerves". Albrecht von Graefes Archiv für Klinische und Experimentelle Ophthalmologie. Albrecht von Graefe's Archive for Clinical and Experimental Ophthalmology. 206 (4): 227–236. doi:10.1007/bf02387334. ISSN 0065-6100. PMID 308327. S2CID 26892630.
- ↑ Wagner, A. "Oculo-auricular phenomenon and its value in neurologic diagnosis".
- ↑ Hackley, Steven A. (2015-10-01). "Evidence for a vestigial pinna-orienting system in humans". Psychophysiology. 52 (10): 1263–1270. doi:10.1111/psyp.12501. ISSN 1469-8986. PMID 26211937.
- ↑ Urban, P. P.; Marczynski, U.; Hopf, H. C. (June 1993). "The oculo-auricular phenomenon. Findings in normals and patients with brainstem lesions". Brain. 116 (3): 727–738. doi:10.1093/brain/116.3.727. ISSN 0006-8950. PMID 8513400.
| | This medical article is a stub. You can help Wikipedia by expanding it. |