Related Research Articles

The lungs are the primary organs of the respiratory system in humans and most other animals, including some snails and a small number of fish. In mammals and most other vertebrates, two lungs are located near the backbone on either side of the heart. Their function in the respiratory system is to extract oxygen from the air and transfer it into the bloodstream, and to release carbon dioxide from the bloodstream into the atmosphere, in a process of gas exchange. The pleurae, which are thin, smooth, and moist, serve to reduce friction between the lungs and chest wall during breathing, allowing for easy and effortless movements of the lungs.

The respiratory system is a biological system consisting of specific organs and structures used for gas exchange in animals and plants. The anatomy and physiology that make this happen varies greatly, depending on the size of the organism, the environment in which it lives and its evolutionary history. In land animals the respiratory surface is internalized as linings of the lungs. Gas exchange in the lungs occurs in millions of small air sacs; in mammals and reptiles these are called alveoli, and in birds they are known as atria. These microscopic air sacs have a very rich blood supply, thus bringing the air into close contact with the blood. These air sacs communicate with the external environment via a system of airways, or hollow tubes, of which the largest is the trachea, which branches in the middle of the chest into the two main bronchi. These enter the lungs where they branch into progressively narrower secondary and tertiary bronchi that branch into numerous smaller tubes, the bronchioles. In birds the bronchioles are termed parabronchi. It is the bronchioles, or parabronchi that generally open into the microscopic alveoli in mammals and atria in birds. Air has to be pumped from the environment into the alveoli or atria by the process of breathing which involves the muscles of respiration.

The thoracic cavity is the chamber of the body of vertebrates that is protected by the thoracic wall. The central compartment of the thoracic cavity is the mediastinum. There are two openings of the thoracic cavity, a superior thoracic aperture known as the thoracic inlet and a lower inferior thoracic aperture known as the thoracic outlet.

The pleural cavity, pleural space, or interpleural space is the potential space between the pleurae of the pleural sac that surrounds each lung. A small amount of serous pleural fluid is maintained in the pleural cavity to enable lubrication between the membranes, and also to create a pressure gradient.
Diffusing capacity of the lung (DL) measures the transfer of gas from air in the lung, to the red blood cells in lung blood vessels. It is part of a comprehensive series of pulmonary function tests to determine the overall ability of the lung to transport gas into and out of the blood. DL, especially DLCO, is reduced in certain diseases of the lung and heart. DLCO measurement has been standardized according to a position paper by a task force of the European Respiratory and American Thoracic Societies.

The thorax or chest is a part of the anatomy of humans, mammals, and other tetrapod animals located between the neck and the abdomen. In insects, crustaceans, and the extinct trilobites, the thorax is one of the three main divisions of the creature's body, each of which is in turn composed of multiple segments.

The thoracic diaphragm, or simply the diaphragm, is a sheet of internal skeletal muscle in humans and other mammals that extends across the bottom of the thoracic cavity. The diaphragm is the most important muscle of respiration, and separates the thoracic cavity, containing the heart and lungs, from the abdominal cavity: as the diaphragm contracts, the volume of the thoracic cavity increases, creating a negative pressure there, which draws air into the lungs. Its high oxygen consumption is noted by the many mitochondria and capillaries present; more than in any other skeletal muscle.

A plethysmograph is an instrument for measuring changes in volume within an organ or whole body. The word is derived from the Greek "plethysmos", and "graphein".
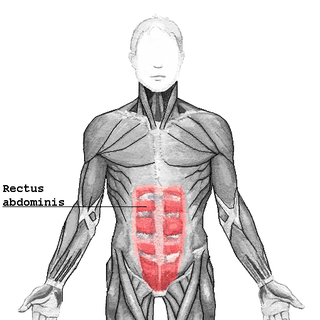
The rectus abdominis muscle, also known as the "abdominal muscle" or simply the "abs", is a pair of segmented skeletal muscle on the ventral aspect of a person's abdomen. The paired muscles are separated at the midline by a band of dense connective tissue called the linea alba, and the connective tissue defining each lateral margin of the rectus abdominus is the linea semilunaris. The muscle extends from the pubic symphysis, pubic crest and pubic tubercle inferiorly, to the xiphoid process and costal cartilages of the 5th–7th ribs superiorly.

Lymphangioleiomyomatosis (LAM) is a rare, progressive and systemic disease that typically results in cystic lung destruction. It predominantly affects women, especially during childbearing years. The term sporadic LAM is used for patients with LAM not associated with tuberous sclerosis complex (TSC), while TSC-LAM refers to LAM that is associated with TSC.

A hemothorax is an accumulation of blood within the pleural cavity. The symptoms of a hemothorax may include chest pain and difficulty breathing, while the clinical signs may include reduced breath sounds on the affected side and a rapid heart rate. Hemothoraces are usually caused by an injury, but they may occur spontaneously due to cancer invading the pleural cavity, as a result of a blood clotting disorder, as an unusual manifestation of endometriosis, in response to Pneumothorax, or rarely in association with other conditions.

The abdominal internal oblique muscle, also internal oblique muscle or interior oblique, is an abdominal muscle in the abdominal wall that lies below the external oblique muscle and just above the transverse abdominal muscle.

Flail chest is a life-threatening medical condition that occurs when a segment of the rib cage breaks due to trauma and becomes detached from the rest of the chest wall. Two of the symptoms of flail chest are chest pain and shortness of breath.

Functional residual capacity (FRC) is the volume of air present in the lungs at the end of passive expiration. At FRC, the opposing elastic recoil forces of the lungs and chest wall are in equilibrium and there is no exertion by the diaphragm or other respiratory muscles.
A pulmonary contusion, also known as lung contusion, is a bruise of the lung, caused by chest trauma. As a result of damage to capillaries, blood and other fluids accumulate in the lung tissue. The excess fluid interferes with gas exchange, potentially leading to inadequate oxygen levels (hypoxia). Unlike pulmonary laceration, another type of lung injury, pulmonary contusion does not involve a cut or tear of the lung tissue.
Hoover's sign in pulmonology is one of two signs named for Charles Franklin Hoover.
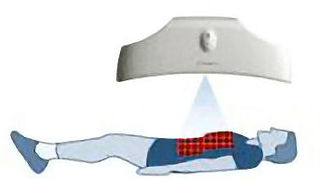
Structured Light Plethysmography (SLP) technology is a noninvasive method for collecting accurate representations of chest and abdominal wall movement. A checkerboard pattern of light is projected from a light projector onto the chest of an individual. Movements of the grid are viewed by two digital cameras, digitalised, and processed to form a 3D model and can be interrogated to assess lung function. The system has been tested on over 70 adults. SLP is simple to use, accurate and cost effective, is self-calibrating and does not require the use of plastic consumables, reducing cost, risk of cross infection and the device's carbon footprint. In conjunction with the Cambridge Veterinary School, proof of concept studies have indicated that the device is sensitive enough to noninvasively pick up respiratory movements in domestic animals.
Respiratory inductance plethysmography (RIP) is a method of evaluating pulmonary ventilation by measuring the movement of the chest and abdominal wall.
Litten's sign, also known as the diaphragm phenomenon, is a paralyzed hemidiaphragm, the portion of the diaphragm in contact with the parietal pleura during respiration in the base of the pleural cavity.

Antonio Pedotti is an Italian scientist, bioengineer and researcher. He is Emeritus Professor of Biomedical Technologies at the Polytechnic University of Milan where he has been chair of the Bioengineering Department, member of the Academic Senate and Director of the Biomedical Technologies Laboratory. He is the former director of the Bioengineering Center of Milan cofounded by the Politecnico and the Scientific Medical Institute Don Gnocchi.
References
- ↑ Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, Pedotti A, Macklem PT, Rochester DF (1996). "Chest wall and lung volume estimation by optical reflectance motion analysis". Journal of Applied Physiology. 81 (6): 2680–9. doi:10.1152/jappl.1996.81.6.2680. PMID 9018522. S2CID 25657044.
- ↑ Aliverti A, Dellacà R, Pelosi P, Chiumello D, Gattinoni L, Pedotti A (2001). "Compartmental analysis of breathing in the supine and prone positions by optoelectronic plethysmography". Annals of Biomedical Engineering. 29 (1): 60–70. doi:10.1114/1.1332084. PMID 11219508. S2CID 23376361.
- ↑ Aliverti A, Cala SJ, Duranti R, Ferrigno G, Kenyon CM, Pedotti A, Scano G, Sliwinski P, Macklem PT, Yan S (1997). "Human respiratory muscle actions and control during exercise". J Appl Physiol. 83 (4): 1256–69. doi:10.1152/jappl.1997.83.4.1256. PMID 9338435. S2CID 14076180.
- ↑ Aliverti A, Stevenson N, Dellacà RL, Lo Mauro A, Pedotti A, Calverley PM (2004). "Regional chest wall volumes during exercise in chronic obstructive pulmonary disease". Thorax. 59 (3): 210–6. doi:10.1136/thorax.2003.011494. PMC 1746979 . PMID 14985554.
- ↑ Lo Mauro A, D'Angelo MG, Romei M, Motta F, Colombo D, Comi GP, Pedotti A, Marchi E, Turconi AC, Bresolin N, Aliverti A (2010). "Abdominal volume contribution to tidal volume as an early indicator of respiratory impairment in Duchenne muscular dystrophy". Eur Respir J. 35 (5): 1118–25. doi: 10.1183/09031936.00037209 . PMID 19840972.
- ↑ Aliverti A, Dellacá R, Pelosi P, Chiumello D, Pedotti A, Gattinoni L (2000). "Optoelectronic plethysmography in intensive care patients". Am J Respir Crit Care Med. 161 (5): 1546–52. doi:10.1164/ajrccm.161.5.9903024. PMID 10806152.