Medicare is the publicly-funded universal health care insurance scheme in Australia, operated by Services Australia. Medicare is the main way Australian citizens and permanent residents access health care in Australia, either partially or fully covering the cost of most primary health care services in the public and private health care system. International visitors from 11 countries have subsidised access to medically necessary treatment under reciprocal agreements. All Australian citizens and permanent residents have access to fully covered health care in public hospitals and clinics.

Medical privacy or health privacy is the practice of maintaining the security and confidentiality of patient records. It involves both the conversational discretion of health care providers and the security of medical records. The terms can also refer to the physical privacy of patients from other patients and providers while in a medical facility. Modern concerns include the degree of disclosure to insurance companies, employers, and other third parties. The advent of electronic medical records (EMR) and patient care management systems (PCMS) have raised new concerns about privacy, balanced with efforts to reduce duplication of services and medical errors.

The Health Insurance Portability and Accountability Act of 1996 was enacted by the 104th United States Congress and signed by President Bill Clinton in 1996. It was created primarily to modernize the flow of healthcare information, stipulate how personally identifiable information maintained by the healthcare and healthcare insurance industries should be protected from fraud and theft, and address limitations on healthcare insurance coverage.

The terms medical record, health record, and medical chart are used somewhat interchangeably to describe the systematic documentation of a single patient's medical history and care across time within one particular health care provider's jurisdiction. The medical record includes a variety of types of "notes" entered over time by health care professionals, recording observations and administration of drugs and therapies, orders for the administration of drugs and therapies, test results, x-rays, reports, etc. The maintenance of complete and accurate medical records is a requirement of health care providers and is generally enforced as a licensing or certification prerequisite.
An electronic health record (EHR) is the systematized collection of patient and population electronically-stored health information in a digital format. These records can be shared across different health care settings. Records are shared through network-connected, enterprise-wide information systems or other information networks and exchanges. EHRs may include a range of data, including demographics, medical history, medication and allergies, immunization status, laboratory test results, radiology images, vital signs, personal statistics like age and weight, and billing information.
A National Provider Identifier (NPI) is a unique 10-digit identification number issued to health care providers in the United States by the Centers for Medicare and Medicaid Services (CMS). The NPI has replaced the unique physician identification number (UPIN) as the required identifier for Medicare services, and is used by other payers, including commercial healthcare insurers. The transition to the NPI was mandated as part of the Administrative Simplifications portion of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
A patient safety organization (PSO) is a group, institution, or association that improves medical care by reducing medical errors. Common functions of patient safety organizations are data collection and analysis, reporting, education, funding, and advocacy.
The Expanded and Improved Medicare for All Act, also known as Medicare for All or United States National Health Care Act, is a bill first introduced in the United States House of Representatives by former Representative John Conyers (D-MI) in 2003, with 25 cosponsors. As of September 26, 2017, it had 120 cosponsors, a majority of Democrats in the House of Representatives, and the highest level of support the bill has received since Conyers began annually introducing the bill in 2003. As of December 6, 2018, the bill's cosponsors had increased to 124.
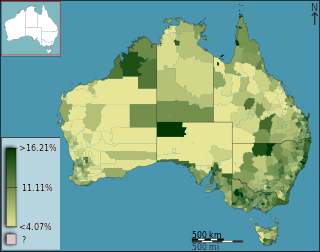
Health care in Australia has a highly developed structure, though because of the nations' vast size, services are not evenly distributed geographically. Health care is delivered in Australia by both government and private companies which are often covered by Medicare. Health care in Australia is largely funded by the government at national, state and local governmental levels, as well as by private health insurance; but the cost of health care is also borne by not-for-profit organisations, with a significant cost being borne by individual patients or by charity. Some services are provided by volunteers, especially remote and mental health services.
Patient portals are healthcare-related online applications that allow patients to interact and communicate with their healthcare providers, such as physicians and hospitals. Typically, portal services are available on the Internet at all hours of the day and night. Some patient portal applications exist as stand-alone web sites and sell their services to healthcare providers. Other portal applications are integrated into the existing web site of a healthcare provider. Still others are modules added onto an existing electronic medical record (EMR) system. What all of these services share is the ability of patients to interact with their medical information via the Internet. Currently, the lines between an EMR, a personal health record, and a patient portal are blurring. For example, Intuit Health and Microsoft HealthVault describe themselves as personal health records (PHRs), but they can interface with EMRs and communicate through the Continuity of Care Record standard, displaying patient data on the Internet so it can be viewed through a patient portal.
Health Information Technology (HIT) is health technology, particularly information technology, applied to health and health care. It supports health information management across computerized systems and the secure exchange of health information between consumers, providers, payers, and quality monitors. Based on an often-cited 2008 report on a small series of studies conducted at four sites that provide ambulatory care – three U.S. medical centers and one in the Netherlands – the use of electronic health records (EHRs) was viewed as the most promising tool for improving the overall quality, safety and efficiency of the health delivery system. According to a 2006 report by the Agency for Healthcare Research and Quality, broad and consistent utilization of HIT will:
popHealth is an open-source reference implementation software tool that automates population health reporting.
An Accountable Care Organization (ACO) is a healthcare organization that ties provider reimbursements to quality metrics and reductions in the cost of care. ACOs in the United States are formed from a group of coordinated health-care practitioners. They use alternative payment models, normally, capitation. The organization is accountable to patients and third-party payers for the quality, appropriateness and efficiency of the health care provided. According to the Centers for Medicare and Medicaid Services, an ACO is "an organization of health care practitioners that agrees to be accountable for the quality, cost, and overall care of Medicare beneficiaries who are enrolled in the traditional fee-for-service program who are assigned to it".
The Health Information Technology for Economic and Clinical Health Act, abbreviated HITECH Act, was enacted under Title XIII of the American Recovery and Reinvestment Act of 2009. Under the HITECH Act, the United States Department of Health and Human Services (U.S.HHS) resolved to spend $25.9 billion to promote and expand the adoption of health information technology. The Washington Post reported the inclusion of "as much as $36.5 billion in spending to create a nationwide network of electronic health records." At the time it was enacted, it was considered "the most important piece of health care legislation to be passed in the last 20 to 30 years" and the "foundation for health care reform."
The National Electronic Health Transition Authority (NEHTA) was established in July 2005 as a collaborative enterprise by the Australian Commonwealth, State and Territory governments to identify and develop the necessary foundations for electronic health (eHealth). NEHTA aims to unlock eHealth system aspects and improve the ways in which information is electronically collected and exchanged.
Health care quality is a level of value provided by any health care resource, as determined by some measurement. As with quality in other fields, it is an assessment of whether something is good enough and whether it is suitable for its purpose. The goal of health care is to provide medical resources of high quality to all who need them; that is, to ensure good quality of life, cure illnesses when possible, to extend life expectancy, and so on. Researchers use a variety of quality measures to attempt to determine health care quality, including counts of a therapy's reduction or lessening of diseases identified by medical diagnosis, a decrease in the number of risk factors which people have following preventive care, or a survey of health indicators in a population who are accessing certain kinds of care.
The Physician Quality Reporting System (PQRS), formerly known as the Physician Quality Reporting Initiative (PQRI), is a health care quality improvement incentive program initiated by the Centers for Medicare and Medicaid Services (CMS) in the United States in 2006. It is an example of a "pay for performance" program which rewards providers financially for reporting healthcare quality data to CMS.
Health care analytics is the health care analysis activities that can be undertaken as a result of data collected from four areas within healthcare; claims and cost data, pharmaceutical and research and development (R&D) data, clinical data, and patient behavior and sentiment data (patient behaviors and preferences,. Health care analytics is a growing industry in the United States, expected to grow to more than $31 billion by 2022. The industry focuses on the areas of clinical analysis, financial analysis, supply chain analysis, as well as marketing, fraud and HR analysis.
Federal and state governments, insurance companies and other large medical institutions are heavily promoting the adoption of electronic health records. The US Congress included a formula of both incentives and penalties for EMR/EHR adoption versus continued use of paper records as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted as part of the, American Recovery and Reinvestment Act of 2009.
The 2018 SingHealth data breach was a data breach incident initiated by unidentified state actors, which happened between 27 June and 4 July 2018. During that period, personal particulars of 1.5 million SingHealth patients and records of outpatient dispensed medicines belonging to 160,000 patients were stolen. Names, National Registration Identity Card (NRIC) numbers, addresses, dates of birth, race, and gender of patients who visited specialist outpatient clinics and polyclinics between 1 May 2015 and 4 July 2018 were maliciously accessed and copied. Information relating to patient diagnosis, test results and doctors' notes were unaffected. Information on Prime Minister Lee Hsien Loong was specifically targeted.