Related Research Articles

Neuropsychology is a branch of psychology concerned with how a person's cognition and behavior are related to the brain and the rest of the nervous system. Professionals in this branch of psychology focus on how injuries or illnesses of the brain affect cognitive and behavioral functions.

Brain injury (BI) is the destruction or degeneration of brain cells. Brain injuries occur due to a wide range of internal and external factors. In general, brain damage refers to significant, undiscriminating trauma-induced damage.
Rehabilitation of sensory and cognitive function typically involves methods for retraining neural pathways or training new neural pathways to regain or improve neurocognitive functioning that have been diminished by disease or trauma. The main objective outcome for rehabilitation is to assist in regaining physical abilities and improving performance. Three common neuropsychological problems treatable with rehabilitation are attention deficit/hyperactivity disorder (ADHD), concussion, and spinal cord injury. Rehabilitation research and practices are a fertile area for clinical neuropsychologists, rehabilitation psychologists, and others.

A concussion, also known as a mild traumatic brain injury (mTBI), is a head injury that temporarily affects brain functioning. Symptoms may include loss of consciousness; memory loss; headaches; difficulty with thinking, concentration, or balance; nausea; blurred vision; dizziness; sleep disturbances, and mood changes. Any of these symptoms may begin immediately, or appear days after the injury. Concussion should be suspected if a person indirectly or directly hits their head and experiences any of the symptoms of concussion. Symptoms of a concussion may be delayed by 1–2 days after the accident. It is not unusual for symptoms to last 2 weeks in adults and 4 weeks in children. Fewer than 10% of sports-related concussions among children are associated with loss of consciousness.
Anosognosia is a condition in which a person with a disability is cognitively unaware of having it due to an underlying physical condition. Anosognosia results from physiological damage to brain structures, typically to the parietal lobe or a diffuse lesion on the fronto-temporal-parietal area in the right hemisphere, and is thus a neuropsychiatric disorder. A deficit of self-awareness, the term was first coined by the neurologist Joseph Babinski in 1914, in order to describe the unawareness of hemiplegia.
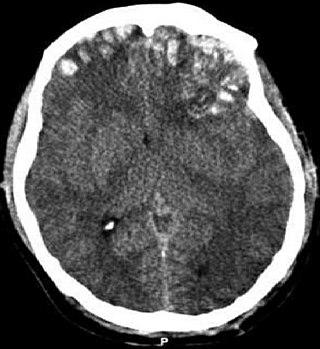
A traumatic brain injury (TBI), also known as an intracranial injury, is an injury to the brain caused by an external force. TBI can be classified based on severity ranging from mild traumatic brain injury (mTBI/concussion) to severe traumatic brain injury. TBI can also be characterized based on mechanism or other features. Head injury is a broader category that may involve damage to other structures such as the scalp and skull. TBI can result in physical, cognitive, social, emotional and behavioral symptoms, and outcomes can range from complete recovery to permanent disability or death.

Acquired brain injury (ABI) is brain damage caused by events after birth, rather than as part of a genetic or congenital disorder such as fetal alcohol syndrome, perinatal illness or perinatal hypoxia. ABI can result in cognitive, physical, emotional, or behavioural impairments that lead to permanent or temporary changes in functioning. These impairments result from either traumatic brain injury or nontraumatic injury derived from either an internal or external source. ABI does not include damage to the brain resulting from neurodegenerative disorders.
Post-concussion syndrome (PCS), also known as persisting symptoms after concussion, is a set of symptoms that may continue for weeks, months, or years after a concussion. PCS is medically classified as a mild traumatic brain injury (TBI). About 35% of people with concussion experience persistent or prolonged symptoms 3 to 6 months after injury. Prolonged concussion is defined as having concussion symptoms for over four weeks following the first accident in youth and for weeks or months in adults.
NEPSY is a series of neuropsychological tests authored by Marit Korkman, Ursula Kirk and Sally Kemp, that is used in various combinations to assess neuropsychological development in children ages 3–16 years in six functional domains.
The Hayling and Brixton tests are neuropsychological tests of executive function created by psychologists Paul W. Burgess and Tim Shallice. It is composed of two tests, the Hayling Sentence Completion Test and the Brixton Spatial Awareness Test.
Post-traumatic amnesia (PTA) is a state of confusion that occurs immediately following a traumatic brain injury (TBI) in which the injured person is disoriented and unable to remember events that occur after the injury. The person may be unable to state their name, where they are, and what time it is. When continuous memory returns, PTA is considered to have resolved. While PTA lasts, new events cannot be stored in the memory. About a third of patients with mild head injury are reported to have "islands of memory", in which the patient can recall only some events. During PTA, the patient's consciousness is "clouded". Because PTA involves confusion in addition to the memory loss typical of amnesia, the term "post-traumatic confusional state" has been proposed as an alternative.
The Rivermead Post-Concussion Symptoms Questionnaire, abbreviated RPQ, is a questionnaire that can be administered to someone who sustains a concussion or other form of traumatic brain injury to measure the severity of symptoms. The RPQ is used to determine the presence and severity of post-concussion syndrome (PCS), a set of somatic, cognitive, and emotional symptoms following traumatic brain injury that may persist anywhere from a week, to months, or even more than six months.

The Trail Making Test is a neuropsychological test of visual attention and task switching. It has two parts, in which the subject is instructed to connect a set of 25 dots as quickly as possible while maintaining accuracy. The test can provide information about visual search speed, scanning, speed of processing, mental flexibility, and executive functioning. It is sensitive to cognitive impairment associated with dementia, including Alzheimer's disease.
The Halstead–Reitan Neuropsychological Test Battery (HRNB) and allied procedures is a comprehensive suite of neuropsychological tests used to assess the condition and functioning of the brain, including etiology, type, localization and lateralization of brain injury. The HRNB was first constructed by Ward C. Halstead, who was chairman of the Psychology Department at the University of Chicago, together with his doctoral student, Ralph Reitan. A major aim of administering the HRNB to patients was if possible to lateralize a lesion to either the left or right cerebral hemisphere by comparing the functioning on both sides of the body on a variety of tests such as the Suppression or Sensory Imperception Test, the Finger Agnosia Test, Finger Tip Writing, the Finger Tapping Test, and the Tactual Performance Test. One difficulty with the HRNB was its excessive administration time. In particular, administration of the Halstead Category Test was lengthy, so subsequent attempts were made to construct reliable and valid short-forms.
The Luria–Nebraska Neuropsychological Battery (LNNB) is a standardized test that identifies neuropsychological deficiencies by measuring functioning on fourteen scales. It evaluates learning, experience, and cognitive skills. The test was created by Charles Golden in 1981 and based on previous work by Alexander Luria that emphasizes a qualitative instead of quantitative approach. The original, adult version is for use with ages fifteen and over, while the Luria–Nebraska Neuropsychological Battery for Children (LNNB-C) can be used with ages eight to twelve; both tests take two to three hours to administer. The LNNB has 269 items divided among fourteen scales, which are motor, rhythm, tactile, visual, receptive speech, expressive speech, writing, reading, arithmetic, memory, intellectual processes, pathognomonic, left hemisphere, and right hemisphere. The test is graded on scales that are correlated to regions of the brain to help identify which region may be damaged. The Luria–Nebraska has been found to be reliable and valid; it is comparable in this sense to other neuropsychological tests in its ability to differentiate between brain damage and mental illness. The test is used to diagnose and determine the nature of cognitive impairment, including the location of the brain damage, to understand the patient's brain structure and abilities, to pinpoint causes of behavior, and to help plan treatment.
Automated Neuropsychological Assessment Metrics (ANAM) is a library of computer-based assessments of cognitive domains including attention, concentration, reaction time, memory, processing speed, and decision-making. ANAM has been administered nearly two million times in a variety of applications and settings. ANAM provides clinicians and researchers with tests to evaluate changes in an individual’s cognitive status over time.

The Corsi block-tapping test is a psychological test that assesses visuo-spatial short term working memory. It involves mimicking a researcher as they tap a sequence of up to nine identical spatially separated blocks. The sequence starts out simple, usually using two blocks, but becomes more complex until the subject's performance suffers. This number is known as the Corsi Span, and average is about 5–6 for typically 'normal' human subjects.
The Delis–Kaplan Executive Function System (D-KEFS) is a neuropsychological test used to measure a variety of verbal and nonverbal executive functions for both children and adults. This assessment was developed over the span of a decade by Dean Delis, Edith Kaplan, and Joel Kramer, and it was published in 2001. The D-KEFS comprises nine tests that were designed to stand alone. Therefore, there are no aggregate measures or composite scores for an examinee's performance. A vast majority of these tests are modified, pre-existing measures ; however, some of these measures are new indices of executive functions.
A pediatric concussion, also known as pediatric mild traumatic brain injury (mTBI), is a head trauma that impacts the brain capacity. Concussion can affect functional, emotional, cognitive and physical factors and can occur in people of all ages. Symptoms following after the concussion vary and may include confusion, disorientation, lightheadedness, nausea, vomiting, blurred vision, loss of consciousness (LOC) and environment sensitivity. Concussion symptoms may vary based on the type, severity and location of the head injury. Concussion symptoms in infants, children, and adolescents often appear immediately after the injury, however, some symptoms may arise multiple days following the injury leading to a concussion. The majority of pediatric patients recover from the symptoms within one month following the injury. 10-30% of children and adolescents have a higher risk of a delayed recovery or of experiencing concussion symptoms that are persisting.
Makarena Diana Dudley, also known as Margaret Dudley, is a New Zealand clinical psychologist, neuropsychologist and academic, specialising in neuropsychology, dementia and Māori health psychology research. She is currently one of the co-directors of the clinical psychology programme at the University of Auckland. In 2016, Dudley became the first permanent Māori clinical psychology lecturer employed at the University of Auckland. Dudley's iwi include Te Rarawa, Te Aupōuri and Ngāti Kahu.
References
- ↑ Collyer CE, Broadbent HA, Church RM (1994). "Preferred rates of repetitive tapping and categorical time production". Perception & Psychophysics. 55 (4): 443–453. doi: 10.3758/bf03205301 . PMID 8036123.
- ↑ Liu W, Forrester L, Whitall J (2006). "A note on time-frequency analysis of finger tapping". Journal of Motor Behavior. 38 (1): 18–28. doi:10.3200/JMBR.38.1.18-28. PMC 2670435 . PMID 16436360.
- ↑ Geldmacher DS, Hills EC (1997). "Effect of stimulus number, target-to-distractor ratio, and motor speed on visual spatial search quality following traumatic brain injury". Brain Injury. 11 (1): 59–66. doi:10.1080/026990597123818. PMID 9012552.
- 1 2 3 Haaland KY, Temkin N, Randahl G, Dikmen S (1994). "Recovery of simple motor skills after head injury". Journal of Clinical and Experimental Neuropsychology. 16 (3): 448–456. doi:10.1080/01688639408402655. PMID 7929712.
- ↑ Hills EC, Geldmacher DS (1998). "The effect of character and array type on visual spatial search acuity following traumatic brain injury". Brain Injury. 12: 69–76. doi:10.1080/026990598122872. PMID 9483339.
- ↑ Prigatano GP, Borgaro SR (2003). "Qualitative features of finger movement during the Halstead finger oscillation test following traumatic brain injury". Journal of the International Neuropsychological Society. 9 (6): 128–133. doi:10.1017/s1355617703000134. PMID 12570365. S2CID 232345145.
- ↑ Murelius O, Haglund Y (1991). "Does Swedish amateur boxing lead to chronic brain damage? A retrospective neuropsychological study". Acta Neurologica Scandinavica. 83 (1): 9–13. doi: 10.1111/j.1600-0404.1991.tb03952.x . PMID 2011947. S2CID 31685414.
- ↑ Dikmen SS, Machamer JE, Winn HR, Temkin NR (1995). "Neuropsychological outcome at 1-year post head injury". Neuropsychology. 9: 80–90. doi:10.1037/0894-4105.9.1.80.