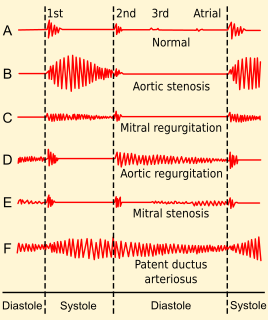
Aortic stenosis is the narrowing of the exit of the left ventricle of the heart, such that problems result. It may occur at the aortic valve as well as above and below this level. It typically gets worse over time. Symptoms often come on gradually with a decreased ability to exercise often occurring first. If heart failure, loss of consciousness, or heart related chest pain occur due to AS the outcomes are worse. Loss of consciousness typically occurs with standing or exercising. Signs of heart failure include shortness of breath especially when lying down, at night, or with exercise, and swelling of the legs. Thickening of the valve without narrowing is known as aortic sclerosis.

A heart valve is a one-way valve that allows blood to flow in one direction through the chambers of the heart. Four valves are usually present in a mammalian heart and together they determine the pathway of blood flow through the heart. A heart valve opens or closes according to differential blood pressure on each side.

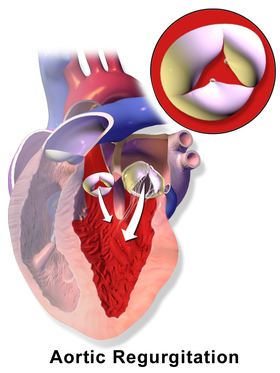
The aortic valve is a valve in the heart of humans and most other animals, located between the left ventricle and the aorta. It is one of the four valves of the heart and one of the two semilunar valves, the other being the pulmonary valve. The aortic valve normally has three cusps or leaflets, although in 1–2% of the population it is found to congenitally have two leaflets. The aortic valve is the last structure in the heart the blood travels through before stopping the flow through the systemic circulation.
The mitral valve, also known as the bicuspid valve or left atrioventricular valve, is one of the four heart valves. It has two cusps or flaps and lies between the left atrium and the left ventricle of the heart. The heart valves are all one-way valves allowing blood flow in just one direction. The mitral valve and the tricuspid valve are known as the atrioventricular valves because they lie between the atria and the ventricles.

Aortic dissection (AD) occurs when an injury to the innermost layer of the aorta allows blood to flow between the layers of the aortic wall, forcing the layers apart. In most cases, this is associated with a sudden onset of severe chest or back pain, often described as "tearing" in character. Also, vomiting, sweating, and lightheadedness may occur. Other symptoms may result from decreased blood supply to other organs, such as stroke, lower extremity ischemia, or mesenteric ischemia. Aortic dissection can quickly lead to death from insufficient blood flow to the heart or complete rupture of the aorta.

Bicuspid aortic valve is a form of heart disease in which two of the leaflets of the aortic valve fuse during development in the womb resulting in a two-leaflet (bicuspid) valve instead of the normal three-leaflet (tricuspid) valve. BAV is the most common cause of heart disease present at birth and affects approximately 1.3% of adults. Normally, the mitral valve is the only bicuspid valve and this is situated between the heart's left atrium and left ventricle. Heart valves play a crucial role in ensuring the unidirectional flow of blood from the atrium to the ventricles, or from the ventricle to the aorta or pulmonary trunk. BAV is normally inherited.
Aortic valve replacement is a procedure whereby the failing aortic valve of a patient's heart is replaced with an artificial heart valve. The aortic valve may need to be replaced because:
A transthoracic echocardiogram (TTE) is the most common type of echocardiogram, which is a still or moving image of the internal parts of the heart using ultrasound. In this case, the probe is placed on the chest or abdomen of the subject to get various views of the heart. It is used as a non-invasive assessment of the overall health of the heart, including a patient's heart valves and degree of heart muscle contraction. The images are displayed on a monitor for real-time viewing and then recorded.
Valvular heart disease is any cardiovascular disease process involving one or more of the four valves of the heart. These conditions occur largely as a consequence of aging, but may also be the result of congenital (inborn) abnormalities or specific disease or physiologic processes including rheumatic heart disease and pregnancy.
Cor triatriatum is a congenital heart defect where the left atrium or right atrium is subdivided by a thin membrane, resulting in three atrial chambers.

Arterial switch operation (ASO) or arterial switch, is an open heart surgical procedure used to correct dextro-transposition of the great arteries (d-TGA); its development was pioneered by Canadian cardiac surgeon William Mustard and it was named for Brazilian cardiac surgeon Adib Jatene, who was the first to use it successfully. It was the first method of d-TGA repair to be attempted, but the last to be put into regular use because of technological limitations at the time of its conception.
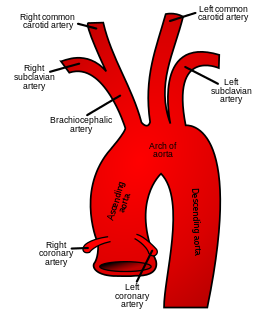
The ascending aorta (AAo) is a portion of the aorta commencing at the upper part of the base of the left ventricle, on a level with the lower border of the third costal cartilage behind the left half of the sternum.
The Dor procedure is a medical technique used as part of heart surgery and originally introduced by the French cardiac surgeon Vincent Dor (b.1932). It is also known as endoventricular circular patch plasty (EVCPP).
Valve-sparing aortic root replacement is a cardiac surgery procedure which is used to treat Aortic aneurysms and to prevent Aortic dissection. It involves replacement of the aortic root without replacement of the aortic valve. Two similar procedures were developed, one by Sir Magdi Yacoub, and another by Tirone David.
The Bentall procedure is a type of cardiac surgery involving composite graft replacement of the aortic valve, aortic root, and ascending aorta, with re-implantation of the coronary arteries into the graft. This operation is used to treat combined disease of the aortic valve and ascending aorta, including lesions associated with Marfan syndrome. The Bentall procedure was first described in 1968 by Hugh Bentall and Antony De Bono. It is considered a standard for individuals who require aortic root replacement, and the vast majority of individuals who undergo the surgery receive mechanical valves.
The following outline is provided as an overview of and topical guide to cardiology, the branch of medicine dealing with disorders of the human heart. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease and electrophysiology. Physicians who specialize in cardiology are called cardiologists.

Apicoaortic Conduit (AAC), also known as Aortic Valve Bypass (AVB), is a cardiothoracic surgical procedure that alleviates symptoms caused by blood flow obstruction from the left ventricle of the heart. Left ventricular outflow tract obstruction (LVOTO) is caused by narrowing of the aortic valve and other valve disorders. AAC, or AVB, relieves the obstruction to blood flow by adding a bioprosthetic valve to the circulatory system to decrease the load on the aortic valve. When an apicoaortic conduit is implanted, blood continues to flow from the heart through the aortic valve. In addition, blood flow bypasses the native valve and exits the heart through the implanted valved conduit. The procedure is effective at relieving excessive pressure gradient across the natural valve. High pressure gradient across the aortic valve can be congenital or acquired. A reduction in pressure gradient results in relief of symptoms.
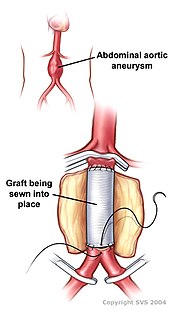
Open aortic surgery (OAS), also known as open aortic repair (OAR), describes a technique whereby an abdominal, thoracic or retroperitoneal surgical incision is used to visualize and control the aorta for purposes of treatment, usually by the replacement of the affected segment with a prosthetic graft. OAS is used to treat aneurysms of the abdominal and thoracic aorta, aortic dissection, acute aortic syndrome, and aortic ruptures. Aortobifemoral bypass is also used to treat atherosclerotic disease of the abdominal aorta below the level of the renal arteries. In 2003, OAS was surpassed by endovascular aneurysm repair (EVAR) as the most common technique for repairing abdominal aortic aneurysms in the United States.

Hans-Joachim Schäfers is a German surgeon, as well as cardiac, thoracic, and vascular surgeon and university professor. He is director of the department of Thoracic and Cardiovascular Surgery at the Saarland University Medical Center in Homburg/Saar, Germany. He is known for his activities in aortic valve repair, aortic surgery, and pulmonary endarterectomy.