Causes and origins of Tourette syndrome have not been fully elucidated. Tourette syndrome (abbreviated as Tourette's or TS) is an inheritedneurodevelopmental disorder that begins in childhood or adolescence, characterized by the presence of multiple motor tics and at least one phonic tic, which characteristically wax and wane. Tourette's syndrome occurs along a spectrum of tic disorders, which includes transient tics and chronic tics.[1][2]
The exact cause of Tourette's is unknown, but it is well established that both genetic and environmental factors are involved.[3] The overwhelming majority of cases of Tourette's are inherited, although the exact mode of inheritance is not yet known,[4] and no gene has been identified.[5] Tics are believed to result from dysfunction in the thalamus, basal ganglia, and frontal cortex of the brain,[3] involving abnormal activity of the brain chemical, or neurotransmitter, dopamine. In addition to dopamine, multiple neurotransmitters, like serotonin, GABA, glutamate, and histamine (H3-receptor), are involved.[6]
Non-genetic factors—while not causing Tourette's—can influence the severity of the disorder. Some forms of Tourette's may be genetically linked to obsessive-compulsive disorder (OCD), while the relationship between Tourette's and attention-deficit hyperactivity disorder (ADHD) is not yet fully understood.
Genetic factors
The exact cause of Tourette's is unknown, but it is well established that both genetic and environmental factors are involved.[7][8][9]Genetic epidemiology studies have shown that Tourette's is highly heritable,[10] and 10 to 100 times more likely to be found among close family members than in the general population.[11] The exact mode of inheritance is not known; no single gene has been identified, and hundreds of genes are likely involved.[10][11][12]Genome-wide association studies were published in 2013[13] and 2015[8] in which no finding reached a threshold for significance.[13]Twin studies show that 50 to 77% of identical twins share a TS diagnosis, while only 10 to 23% of fraternal twins do.[7] But not everyone who inherits the genetic vulnerability will show symptoms.[14][15] A few rare highly penetrant genetic mutations have been found that explain only a small number of cases in single families (the SLITRK1, HDC, and CNTNAP2 genes).[16]
In some cases, tics may not be inherited; these cases are identified as "sporadic" Tourette syndrome (also known as tourettism) because a genetic link is missing.[17]
A person with Tourette syndrome has about a 50% chance of passing the gene(s) to one of their children. Gender appears to have a role in the expression of the genetic vulnerability, with males more likely to express tics than females.[5] Tourette syndrome is a condition of incomplete penetrance, meaning not everyone who inherits the genetic vulnerability will show symptoms. Tourette's also shows variable expression—even family members with the same genetic makeup may show different levels of symptom severity. The gene(s) may express as Tourette syndrome, as a milder tic disorder (transient or chronic tics), or as obsessive compulsive symptoms with no tics at all.[18] Only a minority of the children who inherit the gene(s) will have symptoms severe enough to require medical attention.[19] There is currently no way to predict the symptoms a child may display, even if the gene(s) are inherited.
Recent research suggests that a small number of Tourette syndrome cases may be caused by a defect on chromosome 13 of gene SLITRK1. Some cases of tourettism (tics due to reasons other than inherited Tourette's syndrome) can be caused by mutation.[17] The finding of a chromosomal abnormality appears to apply to a very small minority of cases (1–2%).
Multiple neurotransmitters, like histamine (H3R), dopamine, serotonin, GABA and glutamate are involved in the etiology.[6] After 2010, the central role of histamine (H3-receptor in the basal ganglia) came into focus in the pathophysiology of Tourette syndrome.[29] The striatum is the main input nucleus of the basal ganglia circuit in the disorder, which is linked to the involvement of the histaminergic H3-receptor.[30]
Non-genetic influences
Psychosocial or other non-genetic factors—while not causing Tourette's—can affect the severity of TS in vulnerable individuals and influence the expression of the inherited genes.[31][5][9][11] Pre-natal and peri-natal events increase the risk that a tic disorder or comorbid OCD will be expressed in those with the genetic vulnerability. These include paternal age; forceps delivery; stress or severe nausea during pregnancy; and use of tobacco, caffeine, alcohol,[31] and cannabis during pregnancy.[13] Babies who are born premature with low birthweight, or who have low Apgar scores, are also at increased risk; in premature twins, the lower birthweight twin is more likely to develop TS.[31]
Autoimmune processes may affect the onset of tics or exacerbate them. Both OCD and tic disorders are hypothesized to arise in a subset of children as a result of a post-streptococcal autoimmune process.[32] Its potential effect is described by the controversial hypothesis called PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections), which proposes five criteria for diagnosis in children.[33][34][35] PANDAS and the newer PANS (pediatric acute-onset neuropsychiatric syndrome) hypotheses are the focus of clinical and laboratory research, but remain unproven. There is also a broader hypothesis that links immune-system abnormalities and immune dysregulation with TS.[8][32]
Relation with OCD and ADHD
Some forms of OCD may be genetically linked to Tourette's,[36] although the genetic factors in OCD with and without tics may differ.[7] The genetic relationship of ADHD to Tourette syndrome, however, has not been fully established.[37][38][39] A genetic link between autism and Tourette's has not been established as of 2017.[40]
1 2 3 Fernandez TV, State MW, Pittenger C (2018). "Tourette disorder and other tic disorders". In Daniel H. Geschwind, Henry L. Paulson, Christine Klein (eds.). Neurogenetics, Part I (Review). Handbook of Clinical Neurology. Vol.147. Elsevier. pp.343–54. doi:10.1016/B978-0-444-63233-3.00023-3. ISBN9780444632333. PMID29325623.
↑ van de Wetering BJ, Heutink P (May 1993). "The genetics of the Gilles de la Tourette syndrome: a review". J. Lab. Clin. Med. (Review). 121 (5): 638–45. PMID8478592.
↑ van de Wetering BJ, Heutink P (May 1993). "The genetics of the Gilles de la Tourette syndrome: a review". J. Lab. Clin. Med. 121 (5): 638–45. PMID8478592.
1 2 Robertson MM (February 2011). "Gilles de la Tourette syndrome: the complexities of phenotype and treatment". Br J Hosp Med (Lond). 72 (2): 100–07. doi:10.12968/hmed.2011.72.2.100. PMID21378617.
Tourette syndrome or Tourette's syndrome is a common neurodevelopmental disorder that begins in childhood or adolescence. It is characterized by multiple movement (motor) tics and at least one vocal (phonic) tic. Common tics are blinking, coughing, throat clearing, sniffing, and facial movements. These are typically preceded by an unwanted urge or sensation in the affected muscles known as a premonitory urge, can sometimes be suppressed temporarily, and characteristically change in location, strength, and frequency. Tourette's is at the more severe end of a spectrum of tic disorders. The tics often go unnoticed by casual observers.
Coprolalia is involuntary swearing or the involuntary utterance of obscene words or socially inappropriate and derogatory remarks. The word comes from the Greek κόπρος, meaning "dung, feces", and λαλιά "speech", from λαλεῖν "to talk".
A tic is a sudden and repetitive motor movement or vocalization that is not rhythmic and involves discrete muscle groups. It is typically brief, and may resemble a normal behavioral characteristic or gesture.
The Jumping Frenchmen of Maine were a group of 19th-century lumberjacks who exhibited a rare disorder of unknown origin. The syndrome entails an exaggerated startle reflex which may be described as an uncontrollable "jump"; individuals with this condition can exhibit sudden movements in all parts of the body. Jumping Frenchmen syndrome shares some symptoms with other startle disorders.
Histamine H3 receptors are expressed in the central nervous system and to a lesser extent the peripheral nervous system, where they act as autoreceptors in presynaptic histaminergic neurons and control histamine turnover by feedback inhibition of histamine synthesis and release. The H3 receptor has also been shown to presynaptically inhibit the release of a number of other neurotransmitters (i.e. it acts as an inhibitory heteroreceptor) including, but probably not limited to dopamine, GABA, acetylcholine, noradrenaline, histamine and serotonin.
Palilalia, a complex tic, is a language disorder characterized by the involuntary repetition of syllables, words, or phrases. It has features resembling other complex tics such as echolalia or coprolalia, but, unlike other aphasias, palilalia is based upon contextually correct speech.
Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) is a controversial hypothetical diagnosis for a subset of children with rapid onset of obsessive-compulsive disorder (OCD) or tic disorders. Symptoms are proposed to be caused by group A streptococcal (GAS), and more specifically, group A beta-hemolytic streptococcal (GABHS) infections. OCD and tic disorders are hypothesized to arise in a subset of children as a result of a post-streptococcal autoimmune process. The proposed link between infection and these disorders is that an autoimmune reaction to infection produces antibodies that interfere with basal ganglia function, causing symptom exacerbations, and this autoimmune response results in a broad range of neuropsychiatric symptoms.
Tic disorders are defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM) based on type and duration of tics. Tic disorders are defined similarly by the World Health Organization.
Societal and cultural aspects of Tourette syndrome include legal advocacy and health insurance issues, awareness of notable individuals with Tourette syndrome, and treatment of TS in the media and popular culture.
Tourette syndrome is an inherited neurodevelopmental disorder that begins in childhood or adolescence, characterized by the presence of motor and phonic tics. The management of Tourette syndrome has the goal of managing symptoms to achieve optimum functioning, rather than eliminating symptoms; not all persons with Tourette's require treatment, and there is no cure or universally effective medication. Explanation and reassurance alone are often sufficient treatment; education is an important part of any treatment plan.
Tourettism refers to the presence of Tourette-like symptoms in the absence of Tourette syndrome, as the result of other diseases or conditions, known as "secondary causes".
Sensory phenomena are general feelings, urges or bodily sensations. They are present in many conditions including autism spectrum disorders, epilepsy, neuropathy, obsessive–compulsive disorder, pain conditions, tardive syndromes, and tic disorders.
Habit reversal training (HRT) is a "multicomponent behavioral treatment package originally developed to address a wide variety of repetitive behavior disorders".
Tourette syndrome is an inherited neurological disorder that begins in childhood or adolescence, characterized by the presence of multiple physical (motor) tics and at least one vocal (phonic) tic.
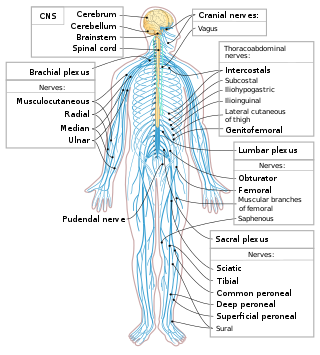
Central nervous system diseases or central nervous system disorders are a group of neurological disorders that affect the structure or function of the brain or spinal cord, which collectively form the central nervous system (CNS). These disorders may be caused by such things as infection, injury, blood clots, age related degeneration, cancer, autoimmune disfunction, and birth defects. The symptoms vary widely, as do the treatments.
Obsessive–compulsive disorder (OCD) is a mental and behavioral disorder in which an individual has intrusive thoughts and feels the need to perform certain routines (compulsions) repeatedly to relieve the distress caused by the obsession, to the extent where it impairs general function.
Basal ganglia disease is a group of physical problems that occur when the group of nuclei in the brain known as the basal ganglia fail to properly suppress unwanted movements or to properly prime upper motor neuron circuits to initiate motor function. Research indicates that increased output of the basal ganglia inhibits thalamocortical projection neurons. Proper activation or deactivation of these neurons is an integral component for proper movement. If something causes too much basal ganglia output, then the ventral anterior (VA) and ventral lateral (VL) thalamocortical projection neurons become too inhibited, and one cannot initiate voluntary movement. These disorders are known as hypokinetic disorders. However, a disorder leading to abnormally low output of the basal ganglia leads to reduced inhibition, and thus excitation, of the thalamocortical projection neurons which synapse onto the cortex. This situation leads to an inability to suppress unwanted movements. These disorders are known as hyperkinetic disorders.
The biology of obsessive–compulsive disorder (OCD) refers biologically based theories about the mechanism of OCD. Cognitive models generally fall into the category of executive dysfunction or modulatory control. Neuroanatomically, functional and structural neuroimaging studies implicate the prefrontal cortex (PFC), basal ganglia (BG), insula, and posterior cingulate cortex (PCC). Genetic and neurochemical studies implicate glutamate and monoamine neurotransmitters, especially serotonin and dopamine.
The cause of obsessive–compulsive disorder is understood mainly through identifying biological risk factors that lead to obsessive–compulsive disorder (OCD) symptomology. The leading hypotheses propose the involvement of the orbitofrontal cortex, basal ganglia, and/or the limbic system, with discoveries being made in the fields of neuroanatomy, neurochemistry, neuroimmunology, neurogenetics, and neuroethology.
A premonitory urge is a sensory phenomenon associated with Tourette syndrome and other tic disorders. Premonitory urges are "uncomfortable feelings or sensations preceding tics that usually are relieved by [a particular] movement".
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.