Related Research Articles

Pneumonia is an inflammatory condition of the lung primarily affecting the small air sacs known as alveoli. Symptoms typically include some combination of productive or dry cough, chest pain, fever, and difficulty breathing. The severity of the condition is variable.

Waterhouse–Friderichsen syndrome (WFS) is defined as adrenal gland failure due to bleeding into the adrenal glands, commonly caused by severe bacterial infection. Typically, it is caused by Neisseria meningitidis.
Atypical pneumonia, also known as walking pneumonia, is any type of pneumonia not caused by one of the pathogens most commonly associated with the disease. Its clinical presentation contrasts to that of "typical" pneumonia. A variety of microorganisms can cause it. When it develops independently from another disease, it is called primary atypical pneumonia (PAP).
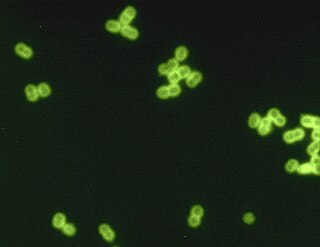
Streptococcus pneumoniae, or pneumococcus, is a Gram-positive, spherical bacteria, alpha-hemolytic member of the genus Streptococcus. They are usually found in pairs (diplococci) and do not form spores and are non motile. As a significant human pathogenic bacterium S. pneumoniae was recognized as a major cause of pneumonia in the late 19th century, and is the subject of many humoral immunity studies.

Pleural empyema is a collection of pus in the pleural cavity caused by microorganisms, usually bacteria. Often it happens in the context of a pneumonia, injury, or chest surgery. It is one of the various kinds of pleural effusion. There are three stages: exudative, when there is an increase in pleural fluid with or without the presence of pus; fibrinopurulent, when fibrous septa form localized pus pockets; and the final organizing stage, when there is scarring of the pleura membranes with possible inability of the lung to expand. Simple pleural effusions occur in up to 40% of bacterial pneumonias. They are usually small and resolve with appropriate antibiotic therapy. If however an empyema develops additional intervention is required.

Haemophilus influenzae is a Gram-negative, non-motile, coccobacillary, facultatively anaerobic, capnophilic pathogenic bacterium of the family Pasteurellaceae. The bacteria are mesophilic and grow best at temperatures between 35 and 37 °C.

Lower respiratory tract infection (LRTI) is a term often used as a synonym for pneumonia but can also be applied to other types of infection including lung abscess and acute bronchitis. Symptoms include shortness of breath, weakness, fever, coughing and fatigue. A routine chest X-ray is not always necessary for people who have symptoms of a lower respiratory tract infection.

Bacterial pneumonia is a type of pneumonia caused by bacterial infection.

The bacterial capsule is a large structure common to many bacteria. It is a polysaccharide layer that lies outside the cell envelope, and is thus deemed part of the outer envelope of a bacterial cell. It is a well-organized layer, not easily washed off, and it can be the cause of various diseases.

Pneumococcal polysaccharide vaccine, sold under the brand name Pneumovax 23, is a pneumococcal vaccine that is used for the prevention of pneumococcal disease caused by the 23 serotypes of Streptococcus pneumoniae contained in the vaccine as capsular polysaccharides. It is given by intramuscular or subcutaneous injection.
Community-acquired pneumonia (CAP) refers to pneumonia contracted by a person outside of the healthcare system. In contrast, hospital-acquired pneumonia (HAP) is seen in patients who have recently visited a hospital or who live in long-term care facilities. CAP is common, affecting people of all ages, and its symptoms occur as a result of oxygen-absorbing areas of the lung (alveoli) filling with fluid. This inhibits lung function, causing dyspnea, fever, chest pains and cough.

Gemifloxacin mesylate, sold under the brand name Factive among others, is a broad-spectrum quinolone antibacterial agent used in the treatment of acute bacterial exacerbation of chronic bronchitis and mild-to-moderate pneumonia. It is taken by mouth. Vansen Pharma Inc. licensed the active ingredient from LG Life Sciences of Korea.

Hospital-acquired pneumonia (HAP) or nosocomial pneumonia refers to any pneumonia contracted by a patient in a hospital at least 48–72 hours after being admitted. It is thus distinguished from community-acquired pneumonia. It is usually caused by a bacterial infection, rather than a virus.

Adenoiditis is the inflammation of the adenoid tissue usually caused by an infection. Adenoiditis is treated using medication or surgical intervention.
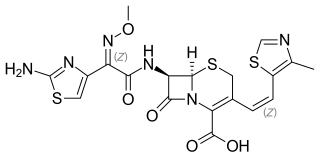
Cefditoren, also known as cefditoren pivoxil is an antibiotic used to treat infections caused by Gram-positive and Gram-negative bacteria that are resistant to other antibiotics. It is mainly used for treatment of community acquired pneumonia. It is taken by mouth and is in the cephalosporin family of antibiotics, which is part of the broader beta-lactam group of antibiotics.

Ceftobiprole, sold under the brand name Zevtera among others, is a fifth-generation cephalosporin antibacterial used for the treatment of hospital-acquired pneumonia and community-acquired pneumonia. It is marketed by Basilea Pharmaceutica under the brand names Zevtera and Mabelio. Like other cephalosporins, ceftobiprole exerts its antibacterial activity by binding to important penicillin-binding proteins and inhibiting their transpeptidase activity which is essential for the synthesis of bacterial cell walls. Ceftobiprole has high affinity for penicillin-binding protein 2a of methicillin-resistant Staphylococcus aureus strains and retains its activity against strains that express divergent mecA gene homologues. Ceftobiprole also binds to penicillin-binding protein 2b in Streptococcus pneumoniae (penicillin-intermediate), to penicillin-binding protein 2x in Streptococcus pneumoniae (penicillin-resistant), and to penicillin-binding protein 5 in Enterococcus faecalis.
Pneumococcal infection is an infection caused by the bacterium Streptococcus pneumoniae.
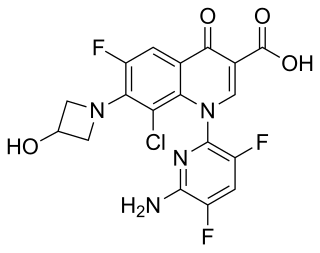
Delafloxacin sold under the brand name Baxdela among others, is a fluoroquinolone antibiotic used to treat acute bacterial skin and skin structure infections.
Claire Veronica Broome is an American epidemiologist, specializing in public health surveillance and vaccine evaluation, who has contributed to the development and effective utilization of key vaccines against pathogens causing pneumonia and meningitis. She joined the Centers for Disease Control and served with the CDC for 28 years, eventually holding the positions of deputy director, acting CDC director (1998), and senior advisor for integrated heath information systems. In 1995 she was promoted to assistant surgeon general in the US Public Health Service.
Necrotizing pneumonia (NP), also known as cavitary pneumonia or cavitatory necrosis, is a rare but severe complication of lung parenchymal infection. In necrotizing pneumonia, there is a substantial liquefaction following death of the lung tissue, which may lead to gangrene formation in the lung. In most cases patients with NP have fever, cough and bad breath, and those with more indolent infections have weight loss. Often patients clinically present with acute respiratory failure. The most common pathogens responsible for NP are Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae. Diagnosis is usually done by chest imaging, e.g. chest X-ray, CT scan. Among these CT scan is the most sensitive test which shows loss of lung architecture and multiple small thin walled cavities. Often cultures from bronchoalveolar lavage and blood may be done for identification of the causative organism(s). It is primarily managed by supportive care along with appropriate antibiotics. However, if patient develops severe complications like sepsis or fails to medical therapy, surgical resection is a reasonable option for saving life.
References
- ↑ Frommer, Myrna; Frommer, Harvey (October 1, 1999). Growing Up Jewish in America: An Oral History. U of Nebraska Press. ISBN 0803269005 – via Google Books.
- 1 2 Narvaez, Alfonso A. (November 22, 1990). "Sidney Musher, 85, Inventor, Executive And Philanthropist". The New York Times– via NYTimes.com.
- 1 2 "Daniel M Musher, M.D." Baylor College of Medicine.
- ↑ "Daniel M Musher, M.D." CARMiG. Archived from the original on 2019-12-27. Retrieved 2019-12-27.
- ↑ "I Remember Mordecai". The Mordecai Kaplan Center for Jewish Peoplehood. 30 July 2023.
- ↑ Schell R, Musher D, Jacobson K, Schwethelm P. Induction of acquired cellular resistance following transfer of thymus-dependent lymphocytes from syphilitic rabbits. J Immunol 1975;114:550-3.
- ↑ Musher DM, McKenzie SO. Infections due to Staphylococcus aureus. Medicine (Baltimore) 1977;56:383-409.
- ↑ Musher DM, Kubitschek KR, Crennan J, Baughn RE. Pneumonia and acute febrile tracheobronchitis due to Haemophilus influenzae. Ann Intern Med 1983;99:444-50.
- ↑ Wallace RJ, Jr., Musher DM. In honor of Dr. Sarah Branham, a star is born. The realization of Branhamella catarrhalis as a respiratory pathogen. Chest 1986;90:447-50.
- ↑ Musher DM, Luchi MJ, Watson DA, Hamilton R, Baughn RE. Pneumococcal polysaccharide vaccine in young adults and older bronchitics: determination of IgG responses by ELISA and the effect of adsorption of serum with non-type-specific cell wall polysaccharide. J Infect Dis 1990;161:728-35.
- ↑ Musher DM, Groover JE, Watson DA, et al. Genetic regulation of the capacity to make immunoglobulin G to pneumococcal capsular polysaccharides. J Investig Med 1997;45:57-68.
- ↑ Musher DM, Rueda AM, Kaka AS, Mapara SM. The association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis 2007;45:158-65.
- ↑ Corrales-Medina VF, Fatemi O, Serpa J, et al. The Association between Staphylococcus aureus bacteremia and acute myocardial infarction. Scand J Infect Dis 2009;In press.
- ↑ Musher DM, Roig IL, Cazares G, Stager CE, Logan N, Safar H. Can an etiologic agent be identified in adults who are hospitalized for community-acquired pneumonia: results of a one-year study. J Infect 2013;67:11-8.
- ↑ Musher DM, Abers MS. Community-Acquired Pneumonia Requiring Hospitalization. N Engl J Med 2015;373:2381.
- ↑ "Daniel M. Musher, MD". Center for Antimicrobial Resistance and Microbial Genomics at McGovern Medical School. Archived from the original on 2019-12-27. Retrieved 2019-12-27.