
An anticoagulant, commonly known as a blood thinner, is a chemical substance that prevents or reduces the coagulation of blood, prolonging the clotting time. Some occur naturally in blood-eating animals, such as leeches and mosquitoes, which help keep the bite area unclotted long enough for the animal to obtain blood.

Coagulation, also known as clotting, is the process by which blood changes from a liquid to a gel, forming a blood clot. It results in hemostasis, the cessation of blood loss from a damaged vessel, followed by repair. The process of coagulation involves activation, adhesion and aggregation of platelets, as well as deposition and maturation of fibrin.
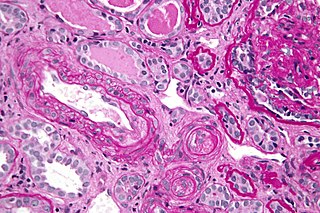
Antiphospholipid syndrome, or antiphospholipid antibody syndrome, is an autoimmune, hypercoagulable state caused by antiphospholipid antibodies. APS can lead to blood clots (thrombosis) in both arteries and veins, pregnancy-related complications, and other symptoms like low platelets, kidney disease, heart disease, and rash. Although the exact etiology of APS is still not clear, genetics is believed to play a key role in the development of the disease. Diagnosis is made based on symptoms and testing, but sometimes research criteria are used to aid in diagnosis. The research criteria for definite APS requires one clinical event and two positive blood test results spaced at least three months apart that detect lupus anticoagulant, anti-apolipoprotein antibodies, and/or anti-cardiolipin antibodies.

The Venereal Disease Research Laboratory test (VDRL) is a blood test for syphilis and related non-venereal treponematoses that was developed by the eponymous US laboratory. The VDRL test is used to screen for syphilis, whereas other, more specific tests are used to diagnose the disease.

The prothrombin time (PT) – along with its derived measures of prothrombin ratio (PR) and international normalized ratio (INR) – is an assay for evaluating the extrinsic pathway and common pathway of coagulation. This blood test is also called protime INR and PT/INR. They are used to determine the clotting tendency of blood, in such things as the measure of warfarin dosage, liver damage, and vitamin K status. PT measures the following coagulation factors: I (fibrinogen), II (prothrombin), V (proaccelerin), VII (proconvertin), and X.

Heparin-induced thrombocytopenia (HIT) is the development of thrombocytopenia, due to the administration of various forms of heparin, an anticoagulant. HIT predisposes to thrombosis. When thrombosis is identified the condition is called heparin-induced thrombocytopenia and thrombosis (HITT). HIT is caused by the formation of abnormal antibodies that activate platelets, which release microparticles that activate thrombin, leading to thrombosis. If someone receiving heparin develops new or worsening thrombosis, or if the platelet count falls, HIT can be confirmed with specific blood tests.

The partial thromboplastin time (PTT), also known as the activated partial thromboplastin time, is a blood test that characterizes coagulation of the blood. A historical name for this measure is the kaolin-cephalin clotting time (KCCT), reflecting kaolin and cephalin as materials historically used in the test. Apart from detecting abnormalities in blood clotting, partial thromboplastin time is also used to monitor the treatment effect of heparin, a widely prescribed drug that reduces blood's tendency to clot.
Mixing studies are tests performed on blood plasma of patients or test subjects to distinguish factor deficiencies from factor inhibitors, such as lupus anticoagulant, or specific factor inhibitors, such as antibodies directed against factor VIII. Mixing studies are screening tests widely performed in coagulation laboratories. The basic purpose of these tests is to determine the cause of prolongation of Prothrombin Time (PT), Partial Thromboplastin Time, or sometimes of thrombin time (TT). Mixing studies take advantage of the fact that factor levels that are 50 percent of normal should give a normal Prothrombin time (PT) or Partial thromboplastin time (PTT) result. Factor deficient plasmas are used in mixing studies. Plasma with known factor deficiencies are commercially available but are very expensive, so they are often prepared in the laboratory and can then be used for mixing tests.
Lupus anticoagulant is an immunoglobulin that binds to phospholipids and proteins associated with the cell membrane. Its name is a partial misnomer, as it is actually a prothrombotic antibody in vivo. The name derives from their properties in vitro, as these antibodies increase coagulation times in laboratory tests such as the activated partial thromboplastin time (aPTT). Investigators speculate that the antibodies interfere with phospholipids used to induce in vitro coagulation. In vivo, the antibodies are thought to interact with platelet membrane phospholipids, increasing adhesion and aggregation of platelets, which accounts for the in vivo prothrombotic characteristics.

Thrombophilia is an abnormality of blood coagulation that increases the risk of thrombosis. Such abnormalities can be identified in 50% of people who have an episode of thrombosis that was not provoked by other causes. A significant proportion of the population has a detectable thrombophilic abnormality, but most of these develop thrombosis only in the presence of an additional risk factor.

Russell's viper is a highly venomous snake in the family Viperidae native to the Indian subcontinent and one of the big four snakes in India. It was described in 1797 by George Shaw and Frederick Polydore Nodder, and named after Patrick Russell, who wrote about it in his 1796 work An account of Indian serpents, collected on the coast of Coromandel.

Protein C deficiency is a rare genetic trait that predisposes to thrombotic disease. It was first described in 1981. The disease belongs to a group of genetic disorders known as thrombophilias. Protein C deficiency is associated with an increased incidence of venous thromboembolism, whereas no association with arterial thrombotic disease has been found.
Catastrophic antiphospholipid syndrome (CAPS), also known as Asherson's syndrome, is a rare autoimmune disease in which widespread, intravascular clotting causes multi-organ failure. The syndrome is caused by antiphospholipid antibodies that target a group of proteins in the body that are associated with phospholipids. These antibodies activate endothelial cells, platelets, and immune cells, ultimately causing a large inflammatory immune response and widespread clotting. CAPS was first described by Ronald Asherson in 1992. The syndrome exhibits thrombotic microangiopathy, multiple organ thromboses, and in some cases tissue necrosis and is considered an extreme or catastrophic variant of the antiphospholipid syndrome.
The thrombin time (TT), also known as the thrombin clotting time (TCT), is a blood test that measures the time it takes for a clot to form in the plasma of a blood sample containing anticoagulant, after an excess of thrombin has been added. It is used to diagnose blood coagulation disorders and to assess the effectiveness of fibrinolytic therapy. This test is repeated with pooled plasma from normal patients. The difference in time between the test and the 'normal' indicates an abnormality in the conversion of fibrinogen to fibrin, an insoluble protein.

Ecarin clotting time (ECT) is a laboratory test used to monitor anticoagulation during treatment with hirudin, an anticoagulant medication which was originally isolated from leech saliva. Ecarin, the primary reagent in this assay, is derived from the venom of the saw-scaled viper, Echis carinatus.
Ecarin is an enzyme that is derived from the venom of the Indian saw-scaled viper, Echis carinatus, It is the primary reagent in the Ecarin clotting time test.

Anti-cardiolipin antibodies (ACA) are antibodies often directed against cardiolipin and found in several diseases, including syphilis, antiphospholipid syndrome, livedoid vasculitis, vertebrobasilar insufficiency, Behçet's syndrome, idiopathic spontaneous abortion, and systemic lupus erythematosus (SLE). They are a form of anti-mitochondrial antibody. In SLE, anti-DNA antibodies and anti-cardiolipin antibodies may be present individually or together; the two types of antibodies act independently. This is in contrast to rheumatoid arthritis with systemic sclerosis (scleroderma) because anti-cardiolipin antibodies are present in both conditions, and therefore may tie the two conditions together.
In autoimmune disease, anti-apolipoprotein H (AAHA) antibodies, also called anti-β2 glycoprotein I antibodies, comprise a subset of anti-cardiolipin antibodies and lupus anticoagulant. These antibodies are involved in sclerosis and are strongly associated with thrombotic forms of lupus. As a result, AAHA are strongly implicated in autoimmune deep vein thrombosis.
Blood clots are a relatively common occurrence in the general population and are seen in approximately 1-2% of the population by age 60. Typically, blood clots develop in the deep veins of the lower extremities, deep vein thrombosis (DVT) or as a blood clot in the lung, pulmonary embolism. A very small number of people who develop blood clots have a more serious and often life-threatening condition, known as thrombotic storm (TS). TS is characterized by the development of more than one blood clot in a short period of time. These clots often occur in multiple and sometimes unusual locations in the body and are often difficult to treat. TS may be associated with an existing condition or situation that predisposes a person to blood clots, such as injury, infection, or pregnancy. In many cases, a risk assessment will identify interventions that will prevent the formation of blood clots.
Kaolin clotting time (KCT) is a sensitive test to detect lupus anticoagulants. There is evidence that suggests it is the most sensitive test for detecting lupus anticoagulants. It can also detect factor VIII inhibitors but is sensitive to unfractionated heparin as well.

