In physiology, nociception, also nocioception; from Latin nocere 'to harm/hurt') is the sensory nervous system's process of encoding noxious stimuli. It deals with a series of events and processes required for an organism to receive a painful stimulus, convert it to a molecular signal, and recognize and characterize the signal to trigger an appropriate defensive response.

Syringomyelia is a generic term referring to a disorder in which a cyst or cavity forms within the spinal cord. Often, syringomyelia is used as a generic term before an etiology is determined. This cyst, called a syrinx, can expand and elongate over time, destroying the spinal cord. The damage may result in loss of feeling, paralysis, weakness, and stiffness in the back, shoulders, and extremities. Syringomyelia may also cause a loss of the ability to feel extremes of hot or cold, especially in the hands. It may also lead to a cape-like bilateral loss of pain and temperature sensation along the upper chest and arms. The combination of symptoms varies from one patient to another depending on the location of the syrinx within the spinal cord, as well as its extent.

Tetraplegia, also known as quadriplegia, is defined as the dysfunction or loss of motor and/or sensory function in the cervical area of the spinal cord. A loss of motor function can present as either weakness or paralysis leading to partial or total loss of function in the arms, legs, trunk, and pelvis. The paralysis may be flaccid or spastic. A loss of sensory function can present as an impairment or complete inability to sense light touch, pressure, heat, pinprick/pain, and proprioception. In these types of spinal cord injury, it is common to have a loss of both sensation and motor control.

The brainstem is the stalk-like part of the brain that connects the forebrain with the spinal cord. In the human brain, the brainstem is composed of the midbrain, the pons, and the medulla oblongata. The midbrain is continuous with the thalamus of the diencephalon through the tentorial notch.

In neuroanatomy, the trigeminal nerve (lit. triplet nerve), also known as the fifth cranial nerve, cranial nerve V, or simply CN V, is a cranial nerve responsible for sensation in the face and motor functions such as biting and chewing; it is the most complex of the cranial nerves. Its name (trigeminal, from Latin tri- 'three' and -geminus 'twin') derives from each of the two nerves (one on each side of the pons) having three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). The ophthalmic and maxillary nerves are purely sensory, whereas the mandibular nerve supplies motor as well as sensory (or "cutaneous") functions. Adding to the complexity of this nerve is that autonomic nerve fibers as well as special sensory fibers (taste) are contained within it.

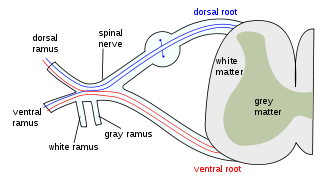
The grey columns are three regions of the somewhat ridge-shaped mass of grey matter in the spinal cord. These regions present as three columns: the anterior grey column, the posterior grey column, and the lateral grey column, all of which are visible in cross-section of the spinal cord.

The spinothalamic tract is a nerve tract in the anterolateral system in the spinal cord. This tract is an ascending sensory pathway to the thalamus. From the ventral posterolateral nucleus in the thalamus, sensory information is relayed upward to the somatosensory cortex of the postcentral gyrus.
The dorsal column–medial lemniscus pathway (DCML) is a sensory pathway of the central nervous system that conveys sensations of fine touch, vibration, two-point discrimination, and proprioception from the skin and joints. It transmits information from the body to the primary somatosensory cortex in the postcentral gyrus of the parietal lobe of the brain. The pathway receives information from sensory receptors throughout the body, and carries this in nerve tracts in the white matter of the dorsal column of the spinal cord to the medulla, where it is continued in the medial lemniscus, on to the thalamus and relayed from there through the internal capsule and transmitted to the somatosensory cortex. The name dorsal-column medial lemniscus comes from the two structures that carry the sensory information: the dorsal columns of the spinal cord, and the medial lemniscus in the brainstem.
Medial medullary syndrome, also known as inferior alternating syndrome, hypoglossal alternating hemiplegia, lower alternating hemiplegia, or Dejerine syndrome, is a type of alternating hemiplegia characterized by a set of clinical features resulting from occlusion of the anterior spinal artery. This results in the infarction of medial part of the medulla oblongata.
Stereognosis is the ability to perceive and recognize the form of an object in the absence of visual and auditory information, by using tactile information to provide cues from texture, size, spatial properties, and temperature, etc. In humans, this sense, along with tactile spatial acuity, vibration perception, texture discrimination and proprioception, is mediated by the dorsal column-medial lemniscus pathway of the central nervous system. Stereognosis tests determine whether or not the parietal lobe of the brain is intact. Typically, these tests involved having the patient identify common objects placed in their hand without any visual cues. Stereognosis is a higher cerebral associative cortical function.

The facial motor nucleus is a collection of neurons in the brainstem that belong to the facial nerve. These lower motor neurons innervate the muscles of facial expression and the stapedius.
Alpha (α) motor neurons (also called alpha motoneurons), are large, multipolar lower motor neurons of the brainstem and spinal cord. They innervate extrafusal muscle fibers of skeletal muscle and are directly responsible for initiating their contraction. Alpha motor neurons are distinct from gamma motor neurons, which innervate intrafusal muscle fibers of muscle spindles.
A syrinx is a rare, fluid-filled neuroglial cavity within the spinal cord (syringomyelia), in the brain stem (syringobulbia), or in the nerves of the elbow, usually in a young age.
Syringobulbia is a medical condition in which syrinxes, or fluid-filled cavities, affect the brainstem. The exact cause is often unknown, but may be linked to a widening of the central canal of the spinal cord. This may affect one or more cranial nerves, resulting in various kinds of facial palsies. Sensory and motor nerve pathways may be affected by interruption or compression of nerves. This disorder is associated with syringomyelia, a syrinx limited to the spinal cord. It can be diagnosed using magnetic resonance imaging. Symptoms may be treated with tricyclic antidepressants.

Subacute combined degeneration of spinal cord, also known as myelosis funiculus, or funicular myelosis, also Lichtheim's disease, and Putnam-Dana syndrome, refers to degeneration of the posterior and lateral columns of the spinal cord as a result of vitamin B12 deficiency (most common). It may also occur similarly as result of vitamin E deficiency, and copper deficiency. It is usually associated with pernicious anemia.

Anterior spinal artery syndrome is syndrome caused by ischemia of the area supplied by the anterior spinal artery, resulting in loss of function of the anterior two-thirds of the spinal cord. The region affected includes the descending corticospinal tract, ascending spinothalamic tract, and autonomic fibers. It is characterized by a corresponding loss of motor function, loss of pain and temperature sensation, and hypotension.
Brown-Séquard syndrome is caused by damage to one half of the spinal cord, i.e. hemisection of the spinal cord resulting in paralysis and loss of proprioception on the same side as the injury or lesion, and loss of pain and temperature sensation on the opposite side as the lesion. It is named after physiologist Charles-Édouard Brown-Séquard, who first described the condition in 1850.

The anterior white commissure is a bundle of nerve fibers which cross the midline of the spinal cord just anterior to the gray commissure. A delta fibers and C fibers carrying pain sensation in the spinothalamic tract contribute to this commissure, as do fibers of the anterior corticospinal tract, which carry motor signals from the primary motor cortex.

The myoclonic triangle is an important feedback circuit of the brainstem and deep cerebellar nuclei which is responsible for modulating spinal cord motor activity.
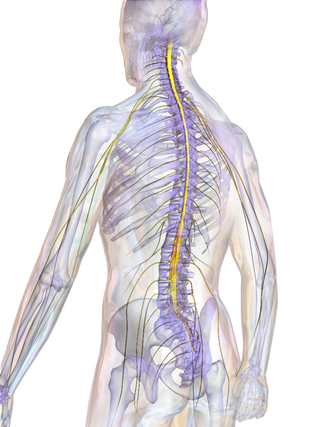
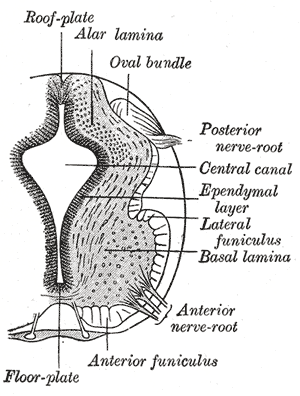
The spinal cord is a long, thin, tubular structure made up of nervous tissue that extends from the medulla oblongata in the brainstem to the lumbar region of the vertebral column (backbone) of vertebrate animals. The center of the spinal cord is hollow and contains a structure called the central canal, which contains cerebrospinal fluid. The spinal cord is also covered by meninges and enclosed by the neural arches. Together, the brain and spinal cord make up the central nervous system.