Equine gastric ulcer syndrome (EGUS) is a common cause of colic and decreased performance in horses. Horses form ulcers in the mucosa of the stomach, leading to pain, decreased appetite, weight loss, and behavioral changes. Treatment generally involves reducing acid production of the stomach and dietary management. Unlike some animals, however, stomach rupture is rare, and the main goal of treating is to reduce pain and improve performance of animals used for showing or racing.
The digestive system of the horse evolved for its grazing lifestyle, where it would almost constantly eat small amounts of roughage throughout the day. Unlike carnivores, who produce stomach acid during meals, horses constantly secrete acid[1] to help digest this source of grass, leading up to 9 gallons produced per day.[2] Unchecked, the stomach acid can lower the pH to levels that will damage the gastric mucosa, leading to ulcers.
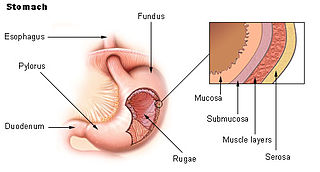
The stomach is divided into two main sections: a squamous region at the upper 1/3 of the stomach near the cardiac sphincter, and a lower glandular region. These two regions are separated by a band of tissue called the margo plicatus. The pH of the stomach contents varies by location. The most dorsal part of the stomach has the highest pH, usually close to 7, dropping to a pH of 3.0–6.0 near the margo plicatus, and reaching as low as 1.5–4.0 in the glandular regions.[1] In foals, pH is uniform since all gastric contents are liquid, and pH rises for a around one hour after milk ingestion.[3]
The esophagus and dorsal stomach is made of stratified squamous epithelium, which is only weakly protected from the effects of hydrochloric acid, and those cells deeper in the layer of tissue transport hydrogen ions intracellularly, leading to death.[1][2] This region is therefore especially vulnerable, and accounts for 80% of all gastric ulcers.[1] The glandular portion produces hydrochloric acid and enzymes such as pepsinogen, as well as bicarbonate and mucus that helps prevent self-digestion.[1][2] Mucosal blood flow is also an important factor in glandular epithelium health, since it provides oxygen and nutrients to the cells and helps to remove excess hydrogen ions.[1]
When a horse is on a diet high in roughage, the fibrous mat of chewed roughage provides a physical barrier and helps prevent splashing of acid up onto the squamous region of the stomach. Additionally, the horse's saliva is alkaline, and provides a chemical buffer that is produced during constant chewing and swallowing.[2]
Both the esophagus and duodenum are also at risk for ulceration. Esophageal ulceration is partially prevented by the tone of the cardia sphincter to prevent reflux, as well as by saliva, which both washes the esophagus and contains mucins that can help protect its surface. The duodenum is protected by its motility which removes HCl, glands in its surface that produce mucins, and products from the pancreas, including bicarbonate, to help neutralize the acidity. Most duodenal ulcers occur in foals, and there appears to be an association between duodenal ulcers and enteritis in these animals.[1] Duodenal ulcers may result in inflammation of the duodenum so profound it blocks gastric emptying, which can cause severe gastric ulcers and occasionally esophageal ulcers. Often this must be treated with a gastrojejunostomy, which is a risky procedure.[3]
Risk factors
Diets high in grain: results in increased serum gastrin secretions and production in volatile fatty acids, and limiting high-carbohydrate feed can help reduce gastric acidity.[3][4]
Diets low in roughage: produce less of a protective fibrous mat of material in the stomach, and requires less chewing and therefore results in less buffering saliva.[2]
Prolonged periods of fasting, due to meal-feeding or anorexia. Fasting has been shown to drop gastric pH to <2, and erosions are found within 48 hours and ulcers within 96 hours of feed deprivation.[1]
Stressful events: including travel, change in environment, and illness.
Confinement: Confinement can, in come cases, increase stress, as horses are prey animals, with a heavy flight-or-fight instinct.[5] Horses moved from pasture to strict stall confinement may be at increased risk of ulceration of the squamous region of the stomach, even with free-choice hay available.[6] Confinement can also result in the development of stereotypical behaviors.[7]
Workload: exercise increases gastric acid production and splashes the gastric contents onto the less-protected squamous portion of the stomach. It also decreases blood flow to the stomach and delays gastric emptying.[2]
Inappropriate use of non-steroidal anti-inflammatory drugs (NSAIDs): NSAIDs decrease the production of prostaglandins, which normally encourage the production of the protective mucus layer of the stomach and allow for normal mucosal blood flow.[1] Inappropriate use of NSAIDs, including excessive doses, prolonged duration of use, or "stacking" (using multiple NSAIDs at once), greatly increases the risks of gastric ulceration in the horse.
Blister beetle toxicity: Cantharidin is caustic to the mucosa of the stomach the chemical
Horses used for competitive activities, such as showing or racing are at greatest risk of gastric ulceration, with up to 60% of show horses, 60–70% of endurance horses, 75% of event horses, and 80–90% of race horses having ulcers.[2][6] These horses have stressful lives compared to non-competitive animals, which includes travel, frequent change of environment, and high workload. Additionally, their diet often consists of a higher proportion of grain relative to roughage, to account for their increased caloric requirements.
Horses undergoing treatment for other medical problems, such as illness or lameness, are also at increased risk, due to the stress of the disease and because they are often confined and placed on long-term non-steroidal anti-inflammatory drugs (NSAIDs).[2]
Foals start secreting hydrochloric acid at two days of age. Nursing has been shown to increase pH, while gastric pH decreases in foals that are recumbent and not sucking regularly.[1] Up to 50% of all foals[8] and 90% of foals in the ICU have ulcers. This may be due to decreased feedings and recumbency.[2] Ulcers in foals are often "silent", producing no clinical signs, and usually occur in the squamous portion of the stomach in animals four months old and younger. Glandular ulcers in foals are thought to be caused by stress, and are often seen in foals four months old and younger that are also sick or debilitated. Clinical ulcers in foals primarily occur in animals < 270 days old, and are usually found on the squamous epithelium of the stomach. Pyloric or duodenal ulcers are rare, and most often seen in animals three to five months of age. Ulcers in these regions are usually asymptomatic, but can cause stricture, leading to gastric outflow obstruction. Perforation secondary to ulcers, although rare, can occur both in the stomach and the duodenum, producing peritonitis. Rupture can not be predicted by ulcer severity as seen on endoscopic examination, and clinical signs are often not present until just prior to the event.[1]
Unlike humans, Helicobacter infection has not been shown to be a definitive cause of gastric ulcers in horses.[9] Although it has not been cultured, DNA from the organism has been found in the gastric mucosa using PCR.[10][11] Additionally, ulcers have been shown to be colonized by bacteria[12] which may prevent healing. Given that some horses do not respond to traditional therapy, it is sometimes recommended to add antibiotics to their treatment regimes.[13]
Clinical signs
The process of gastric ulceration is similar to esophageal reflux in people (heartburn), where acid damages the epithelium of the esophagus. Therefore, behaviors associated to pain are the most common clinical signs of a horse with EGUS. This commonly includes chronic intermittent colic, especially after eating, decreased appetite or sudden cessation of eating in the middle of a meal, weight loss, decreased performance, changes in attitude, and "girthiness". Horses with ulcers may be difficult to keep in good condition, despite a high-quality diet. Additionally, horses may display bruxism, ptyalism, and dullness. Foals may additionally have diarrhea and display a potbelly and poor hair coat.[1][2] Those foals with more serious ulceration are also seen to lay in dorsal recumbency and show pain when palpated just caudal to the xiphoid process.[1]
Horses may not display any clinical signs, even with severe gastric ulcers. However, gastric ulcers are usually more severe in horses displaying clinical signs.[14]
Diagnosis
Diagnosis is often made based on history, clinical signs, and response to treatment, but the best diagnostic tool involves endoscopic visualization of the stomach in a process called gastroscopy. The horse is fasted for at least 6 hours[1] prior to the procedure to help reduce the amount of feed material in the stomach. They are then sedated, and an endoscope is passed through one of the nostrils, into the esophagus, and down to the stomach. The endoscope must be at least 2 meters to visualize the non-glandular region of the stomach, and 2.5–3 meters to visualize the glandular region.[13] This is a simple and minimally invasive procedure that allows for definitive diagnosis and can be used to track healing of lesions once treatment has begun.[2]
Degree of ulceration is graded both on lesion number (grade 0–4, with a grade 4 for stomachs containing >10 lesions or diffuse ulceration) and lesion severity (0-5, with 5 being deep, active, hemorrhagic ulcers). The squamous and glandular regions are graded separately.[15]
Treatment and prevention
The main goal of treatment of horses with gastric ulcers is to keep the pH of the stomach >4.[2] Currently in the US, the only FDA approved method of treatment is through the use of the proton pump inhibitoromeprazole,[2] which has been shown to decrease the secretion of hydrochloric acid.[16] Treatment is expensive and usually requires at least a month of daily administration of the drug. To reduce costs, compounded omeprazole is occasionally used; however, the efficacy of these products are likely poor.[17] Omeprazole requires 3–5 days to reach steady-state levels in horses, so horses suffering from ulcers are often started on H2 antagonists at the same time.[1] For this reason, some veterinarians recommend beginning prophylactic treatment several days before a stressful event. It is best to exercise a horse 2–8 hours after administration of omeprazole, and it may be taken up more quickly if the horse is given a grain meal at the same time, which should improve efficacy.[3]
Prophylactic use of both omeprazole and H2 antagonists such as ranitidine, cimetidine, and famotidine can be used to help prevent gastric ulcer formation when the horse will be placed into a stressful situation, such as travel or showing. Ranitidine has been shown to reduce ulceration when given concurrently during feed deprivation trials.[1] H2 antagonists are cheaper and will decrease stomach acid production but require more frequent administration compared to PPIs, usually every eight hours. There are no studies suggesting that H2 antagonists improve the healing of ulcers already present.[1] H2 antagonists require doses much higher than other species to block acid production in the equine stomach, possibly because so little histamine is needed to produce maximal secretion of acid.[3] This is also true for omeprazole doses, especially if given orally.
Antacids have a short duration of effectiveness, and therefore are not very practical for use in horses because the damaging acid is produced constantly rather than just at meals. Such medications would require prohibitively frequent dosing to treat ulcers in the horse if used independently of other drugs.
Sucralfate is often used as an adjunctive therapy. At a pH <4, it becomes thick in consistency and it binds to gastric ulcerations preferably over squamous epithelial cells. It is not recommended as the sole treatment of EGUS because it has not been shown to have great efficacy in treating ulcers of the squamous region, and has not been studied in cases of glandular ulcers.[1] If it is used, it should not be given around the time of an H2 antagonist, because sucralfate binds best at a lower pH.[3]
Dietary management is critical: increasing roughage provides a physical barrier to help protect the stomach as well as encourages salivation. Horses prone to gastric ulcers should have access to hay or grass as much as possible, ideally constantly, and meal feeding should be kept to a minimum. Specifically, feeding alfalfa hay has also been shown to decrease the severity of ulcers.[18][19] Grain should be reduced to a level below 0.5kg grain/220kg body weight,[4] and ideally as much as possible. Corn oil may be beneficial, especially for horses taking NSAIDs, as it contains 40% linoleic aid, a substance that is thought to increase prostaglandin E2 (one of the protective prostaglandins) and decrease acid production.[3] Additional turnout and a reduction in training or traveling can also have positive effects. Stalled horses should be kept in as stress-free of an environment as possible, with access to hay and the ability to see other horses. NSAID use should be kept to a minimum, and use of COX-2 selective NSAIDs such as firocoxib may be preferable over other commonly used NSAIDs.[2]
Recent studies
Although oral omeprazole treatment is the licensed treatment in the majority of countries, recent studies have shown long‐acting injectable omeprazole has been demonstrated to suppress acid production more markedly, more consistently and for longer than observed in previous investigations using oral omeprazole.[20]
Related Research Articles
Peptic ulcer disease is a break in the inner lining of the stomach, the first part of the small intestine, or sometimes the lower esophagus. An ulcer in the stomach is called a gastric ulcer, while one in the first part of the intestines is a duodenal ulcer. The most common symptoms of a duodenal ulcer are waking at night with upper abdominal pain, and upper abdominal pain that improves with eating. With a gastric ulcer, the pain may worsen with eating. The pain is often described as a burning or dull ache. Other symptoms include belching, vomiting, weight loss, or poor appetite. About a third of older people with peptic ulcers have no symptoms. Complications may include bleeding, perforation, and blockage of the stomach. Bleeding occurs in as many as 15% of cases.
The esophagus or oesophagus, colloquially known also as the food pipe, food tube, or gullet, is an organ in vertebrates through which food passes, aided by peristaltic contractions, from the pharynx to the stomach. The esophagus is a fibromuscular tube, about 25 cm (10 in) long in adults, that travels behind the trachea and heart, passes through the diaphragm, and empties into the uppermost region of the stomach. During swallowing, the epiglottis tilts backwards to prevent food from going down the larynx and lungs. The word oesophagus is from Ancient Greek οἰσοφάγος (oisophágos), from οἴσω (oísō), future form of φέρω + ἔφαγον.
Helicobacter pylori, previously known as Campylobacter pylori, is a gram-negative, flagellated, helical bacterium. Mutants can have a rod or curved rod shape, and these are less effective. Its helical body is thought to have evolved in order to penetrate the mucous lining of the stomach, helped by its flagella, and thereby establish infection. The bacterium was first identified as the causal agent of gastric ulcers in 1983 by the Australian doctors Barry Marshall and Robin Warren.
Coffee ground vomitus refers to a particular appearance of vomit. Within organic heme molecules of red blood cells is the element iron, which oxidizes following exposure to gastric acid. This reaction causes the vomitus to look like ground coffee.
Gastric acid, gastric juice, or stomach acid is a digestive fluid formed within the stomach lining. With a pH between 1 and 3, gastric acid plays a key role in digestion of proteins by activating digestive enzymes, which together break down the long chains of amino acids of proteins. Gastric acid is regulated in feedback systems to increase production when needed, such as after a meal. Other cells in the stomach produce bicarbonate, a base, to buffer the fluid, ensuring a regulated pH. These cells also produce mucus – a viscous barrier to prevent gastric acid from damaging the stomach. The pancreas further produces large amounts of bicarbonate and secretes bicarbonate through the pancreatic duct to the duodenum to neutralize gastric acid passing into the digestive tract.
Esophagogastroduodenoscopy (EGD) or oesophagogastroduodenoscopy (OGD), also called by various other names, is a diagnostic endoscopic procedure that visualizes the upper part of the gastrointestinal tract down to the duodenum. It is considered a minimally invasive procedure since it does not require an incision into one of the major body cavities and does not require any significant recovery after the procedure. However, a sore throat is common.
Gastritis is inflammation of the lining of the stomach. It may occur as a short episode or may be of a long duration. There may be no symptoms but, when symptoms are present, the most common is upper abdominal pain. Other possible symptoms include nausea and vomiting, bloating, loss of appetite and heartburn. Complications may include stomach bleeding, stomach ulcers, and stomach tumors. When due to autoimmune problems, low red blood cells due to not enough vitamin B12 may occur, a condition known as pernicious anemia.
Curling's ulcer is an acute gastric erosion resulting as a complication from severe burns when reduced plasma volume leads to ischemia and cell necrosis (sloughing) of the gastric mucosa. The condition was first described in 1823 and named after Thomas Blizard Curling, who observed ten such patients in 1842.
A Cushing ulcer, named after Harvey Cushing, is a gastric ulcer associated with elevated intracranial pressure. It is also called von Rokitansky–Cushing syndrome. Apart from the stomach, ulcers may also develop in the proximal duodenum and distal esophagus.
Colic in horses is defined as abdominal pain, but it is a clinical symptom rather than a diagnosis. The term colic can encompass all forms of gastrointestinal conditions which cause pain as well as other causes of abdominal pain not involving the gastrointestinal tract. What makes it tricky is that different causes can manifest with similar signs of distress in the animal. Recognizing and understanding these signs is pivotal, as timely action can spell the difference between a brief moment of discomfort and a life-threatening situation. The most common forms of colic are gastrointestinal in nature and are most often related to colonic disturbance. There are a variety of different causes of colic, some of which can prove fatal without surgical intervention. Colic surgery is usually an expensive procedure as it is major abdominal surgery, often with intensive aftercare. Among domesticated horses, colic is the leading cause of premature death. The incidence of colic in the general horse population has been estimated between 4 and 10 percent over the course of the average lifespan. Clinical signs of colic generally require treatment by a veterinarian. The conditions that cause colic can become life-threatening in a short period of time.
Sucralfate, sold under various brand names, is a medication used to treat stomach ulcers, gastroesophageal reflux disease (GERD), radiation proctitis, and stomach inflammation and to prevent stress ulcers. Its usefulness in people infected by H. pylori is limited. It is used by mouth and rectally.
Gastrinomas are neuroendocrine tumors (NETs), usually located in the duodenum or pancreas, that secrete gastrin and cause a clinical syndrome known as Zollinger–Ellison syndrome (ZES). A large number of gastrinomas develop in the pancreas or duodenum, with near-equal frequency, and approximately 10% arise as primary neoplasms in lymph nodes of the pancreaticoduodenal region.
A vagotomy is a surgical procedure that involves removing part of the vagus nerve. It is performed in the abdomen.
A stress ulcer is a single or multiple mucosal defect usually caused by physiological stress which can become complicated by upper gastrointestinal bleeding. These ulcers can be caused by shock, sepsis, trauma or other conditions and are found in patients with chronic illnesses. These ulcers are a significant issue in patients in critical and intensive care.
Troxipide is a drug used in the treatment of gastroesophageal reflux disease. Troxipide is a systemic non-antisecretory gastric cytoprotective agent with anti-ulcer, anti-inflammatory and mucus secreting properties irrespective of pH of stomach or duodenum. Troxipide is currently marketed in Japan (Aplace), China (Shuqi), South Korea (Defensa), and India (Troxip). It is used for the management of gastric ulcers, and amelioration of gastric mucosal lesions in acute gastritis and acute exacerbation of chronic gastritis.
Chromoendoscopy is a medical procedure wherein dyes are instilled into the gastrointestinal tract at the time of visualization with fibre-optic endoscopy. The purposes of chromoendoscopy is chiefly enhance the characterization of tissues, although dyes may be used for other functional purposes. The detail achieved with chromoendoscopy can often allow for identification of the tissue type or pathology based upon the pattern uncovered.
The gastrointestinal wall of the gastrointestinal tract is made up of four layers of specialised tissue. From the inner cavity of the gut outwards, these are the mucosa, the submucosa, the muscular layer and the serosa or adventitia.
The human digestive system consists of the gastrointestinal tract plus the accessory organs of digestion. Digestion involves the breakdown of food into smaller and smaller components, until they can be absorbed and assimilated into the body. The process of digestion has three stages: the cephalic phase, the gastric phase, and the intestinal phase.
Acid peptic diseases, such as peptic ulcers, Zollinger-Ellison syndrome, and gastroesophageal reflux disease, are caused by distinct but overlapping pathogenic mechanisms involving acid effects on mucosal defense. Acid reflux damages the esophageal mucosa and may also cause laryngeal tissue injury, leading to the development of pulmonary symptoms.
Antrectomy, also called distal gastrectomy, is a type of gastric resection surgery that involves the removal of the stomach antrum to treat gastric diseases causing the damage, bleeding, or blockage of the stomach. This is performed using either the Billroth I (BI) or Billroth II (BII) reconstruction method. Quite often, antrectomy is used alongside vagotomy to maximise its safety and effectiveness. Modern antrectomies typically have a high success rate and low mortality rate, but the exact numbers depend on the specific conditions being treated.
↑ Murray, MJ (15 October 1989). "Endoscopic appearance of gastric lesions in foals: 94 cases (1987-1988)". Journal of the American Veterinary Medical Association. 195 (8): 1135–41. PMID2808108.
↑ Husted L et al. Examination of equine glandular stomach lesions for bacteria, including Helicobacter spp by fluorescence in situ hybridisation. BMC Microbiol. 2010 Mar 19;10:84
↑ Contreras, M., A. Morales, M.A. Garcia-Amado, M. De Vera, V. Bermúdez, and P. Gueneau. 2007. Detection of Helicobacter-like DNA in the gastric mucosa of Thoroughbred horses. Lett. Appl. Microbiol. 45:553-557.
↑ Scott, D.R., E.A. Marcus, S.S.P. Shirazi-Beechey, and M. Murray. 2001. Evidence of Helicobacter infection in the horse. In: Proc. Amer. Soc. Microbiologists 287.
↑ Yuki, N., T. Shimazaki, A. Kushiro, K. Watanabe, K. Uchida, T. Yuyama, and M. Morotomi. 2000. Colonization of the stratified squamous epithelium of the nonsecreting area of horse stomach by Lactobacilli. Appl. Environ. Micro. 66: 5030-5034.
↑ Murray MJ et al. (1989) Gastric ulcers in horses: a comparison of endoscopic findings in horses with and without clinical signs. Equine vet J., 68-72.
↑ Andrews FM et al. (1999) Effects of orally administered enteric-coated omeprazole on gastric acid secretion in horses. AJVR, 60, 8, 929-931.
↑ Nieto, J.E., S. Spier, F.S. Pipers, S. Stanley, M.R. Aleman, D.C. Smith, and J.R. Snyder. 2002. Comparison of paste and suspension formulations of omeprazole in the healing of gastric ulcers in racehorses in active training. J. Am. Vet. Med. Assoc. 221:1139-1143.
↑ Nadeau, J.A., F.M. Andrews, and A.G. Matthew. 2000. Evaluation of diet as a cause of gastric ulcers in horses. Am. J. Vet. Res. 61:784-790.
↑ Lybbert, T., P. Gibbs, N. Cohen, B. Scott, and D. Sigler. 2007. Feeding alfalfa hay to exercising horses reduces the severity of gastric squamous mucosal ulceration. In: Proc. Amer. Assoc. Eq. Practnr. 53:525-526.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.