
Polycystic ovary syndrome, or polycystic ovarian syndrome (PCOS), is the most common endocrine disorder in women of reproductive age. The syndrome is named after cysts which form on the ovaries of some people with this condition, though this is not a universal symptom, and not the underlying cause of the disorder.

Cushing's syndrome is a collection of signs and symptoms due to prolonged exposure to glucocorticoids such as cortisol. Signs and symptoms may include high blood pressure, abdominal obesity but with thin arms and legs, reddish stretch marks, a round red face due to facial plethora, a fat lump between the shoulders, weak muscles, weak bones, acne, and fragile skin that heals poorly. Women may have more hair and irregular menstruation. Occasionally there may be changes in mood, headaches, and a chronic feeling of tiredness.

Hirsutism is excessive body hair on parts of the body where hair is normally absent or minimal. The word is from early 17th century: from Latin hirsutus meaning "hairy". It usually refers to a male pattern of hair growth in a female that may be a sign of a more serious medical condition, especially if it develops well after puberty. Cultural stigma against hirsutism can cause much psychological distress and social difficulty. Discrimination based on facial hirsutism often leads to the avoidance of social situations and to symptoms of anxiety and depression.
Anovulation is when the ovaries do not release an oocyte during a menstrual cycle. Therefore, ovulation does not take place. However, a woman who does not ovulate at each menstrual cycle is not necessarily going through menopause. Chronic anovulation is a common cause of infertility.

Acanthosis nigricans is a medical sign characterised by brown-to-black, poorly defined, velvety hyperpigmentation of the skin. It is usually found in body folds, such as the posterior and lateral folds of the neck, the armpits, groin, navel, forehead and other areas.
Adrenarche is an early stage in sexual maturation that happens in some higher primates, typically peaks at around 20 years of age, and is involved in the development of pubic hair, body odor, skin oiliness, axillary hair, sexual attraction/sexual desire/increased libido and mild acne. During adrenarche the adrenal glands secrete increased levels of weak adrenal androgens, including dehydroepiandrosterone (DHEA), dehydroepiandrosterone sulfate (DHEA-S), and androstenedione (A4), but without increased cortisol levels. Adrenarche is the result of the development of a new zone of the adrenal cortex, the zona reticularis. Adrenarche is a process related to puberty, but distinct from hypothalamic–pituitary–gonadal axis maturation and function.
Pubarche refers to the first appearance of pubic hair at puberty and it also marks the beginning of puberty. It is one of the physical changes of puberty and can occur independently of complete puberty. The early stage of sexual maturation, also known as adrenarche, is marked by characteristics including the development of pubic hair, axillary hair, adult apocrine body odor, acne, and increased oiliness of hair and skin. The Encyclopedia of Child and Adolescent Health corresponds SMR2 with pubarche, defining it as the development of pubic hair that occurs at a mean age of 11.6 years in females and 12.6 years in males. It further describes that pubarche's physical manifestation is vellus hair over the labia or the base of the penis. See Table 1 for the entirety of the sexual maturity rating description.

Hyperandrogenism is a medical condition characterized by high levels of androgens. It is more common in women than men. Symptoms of hyperandrogenism may include acne, seborrhea, hair loss on the scalp, increased body or facial hair, and infrequent or absent menstruation. Complications may include high blood cholesterol and diabetes. It occurs in approximately 5% of women of reproductive age.

Flutamide, sold under the brand name Eulexin among others, is a nonsteroidal antiandrogen (NSAA) which is used primarily to treat prostate cancer. It is also used in the treatment of androgen-dependent conditions like acne, excessive hair growth, and high androgen levels in women. It is taken by mouth, usually three times per day.

Pattern hair loss is a hair loss condition that primarily affects the top and front of the scalp. In male-pattern hair loss (MPHL), the hair loss typically presents itself as either a receding front hairline, loss of hair on the crown (vertex) of the scalp, or a combination of both. Female-pattern hair loss (FPHL) typically presents as a diffuse thinning of the hair across the entire scalp.
Rabson–Mendenhall syndrome is a rare autosomal recessive disorder characterized by severe insulin resistance. The disorder is caused by mutations in the insulin receptor gene. Symptoms include growth abnormalities of the head, face and nails, along with the development of acanthosis nigricans. Treatment involves controlling blood glucose levels by using insulin and incorporating a strategically planned, controlled diet. Also, direct actions against other symptoms may be taken This syndrome usually affects children and has a prognosis of 1–2 years.
An androgen-dependent condition, disease, disorder, or syndrome, is a medical condition that is, in part or full, dependent on, or is sensitive to, the presence of androgenic activity in the body.

Aromatase deficiency is a rare condition characterized by extremely low levels or complete absence of the enzyme aromatase activity in the body. It is an autosomal recessive disease resulting from various mutations of gene CYP19 (P450arom) which can lead to ambiguous genitalia and delayed puberty in females, continued linear growth into adulthood and osteoporosis in males and virilization in pregnant mothers. As of 2020, fewer than 15 cases have been identified in genetically male individuals and at least 30 cases in genetically female individuals.
Hyperthecosis, or ovarian hyperthecosis, is hyperplasia of the theca interna of the ovary. Hyperthecosis occurs when an area of luteinization occurs along with stromal hyperplasia. The luteinized cells produce androgens, which may lead to hirsutism and virilization in affected women.
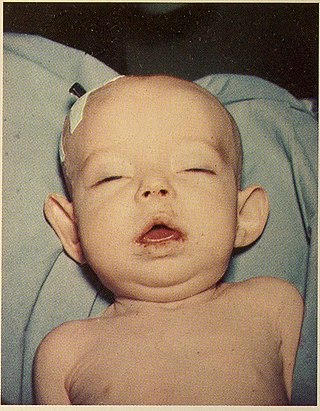
Donohue syndrome is an extremely rare and severe genetic disorder. Leprechaunism derives its name from the hallmark elvish features exhibited by the affected individuals. The disease is caused by a mutation in the INSR gene, which contains the genetic information for the formation of insulin receptors. As a result, affected individuals have either a decreased number of insulin receptors, or insulin receptor with greatly impaired functionality. The lack and impairment of insulin receptor functionality leads to an inability to regulate blood glucose levels through severe insulin resistance. This will ultimately lead to affected development of tissues and organs throughout the body. In addition to the physical abnormalities, leprechaunism is also characterized by endocrine system abnormalities that can lead to conditions such as hyperglycemia, hypoglycemia, hyperinsulemia, and the enlargement of certain sex organs such as the penis in males, and the clitoris in females.

Cyproterone acetate (CPA), sold alone under the brand name Androcur or with ethinylestradiol under the brand names Diane or Diane-35 among others, is an antiandrogen and progestin medication used in the treatment of androgen-dependent conditions such as acne, excessive body hair growth, early puberty, and prostate cancer, as a component of feminizing hormone therapy for transgender individuals, and in birth control pills. It is formulated and used both alone and in combination with an estrogen. CPA is taken by mouth one to three times per day.
Cortisone reductase deficiency is caused by dysregulation of the 11β-hydroxysteroid dehydrogenase type 1 enzyme (11β-HSD1), otherwise known as cortisone reductase, a bi-directional enzyme, which catalyzes the interconversion of cortisone to cortisol in the presence of NADH as a co-factor. If levels of NADH are low, the enzyme catalyses the reverse reaction, from cortisol to cortisone, using NAD+ as a co-factor.
Cortisol is a glucocorticoid that plays a variety of roles in many different biochemical pathways, including, but not limited to: gluconeogenesis, suppressing immune system responses and carbohydrate metabolism.
One of the symptoms of cortisone reductase deficiency is hyperandrogenism, resulting from activation of the Hypothalamic–pituitary–adrenal axis. The deficiency has been known to exhibit symptoms of other disorders such as Polycystic Ovary Syndrome in women. Cortisone Reductase Deficiency alone has been reported in fewer than ten cases in total, all but one case were women. Elevated activity of 11β-HSD1 can lead to obesity or Type II Diabetes, because of the role of cortisol in carbohydrate metabolism and gluconeogenesis.
Obesity is defined as an abnormal accumulation of body fat, usually 20% or more over an individual's ideal body weight. This is often described as a body mass index (BMI) over 30. However, BMI does not account for whether the excess weight is fat or muscle, and is not a measure of body composition. For most people, however, BMI is an indication used worldwide to estimate nutritional status. Obesity is usually the result of consuming more calories than the body needs and not expending that energy by doing exercise. There are genetic causes and hormonal disorders that cause people to gain significant amounts of weight but this is rare. People in the obese category are much more likely to suffer from fertility problems than people of normal healthy weight.

Ethinylestradiol/cyproterone acetate (EE/CPA), also known as co-cyprindiol and sold under the brand names Diane and Diane-35 among others, is a combination of ethinylestradiol (EE), an estrogen, and cyproterone acetate (CPA), a progestin and antiandrogen, which is used as a birth control pill to prevent pregnancy in women. It is also used to treat androgen-dependent conditions in women such as acne, seborrhea, excessive facial/body hair growth, scalp hair loss, and high androgen levels associated with ovaries with cysts. The medication is taken by mouth once daily for 21 days, followed by a 7-day free interval.

Generalized glucocorticoid resistance or Chrousos syndrome is a rare genetic disorder that can run in families or be sporadic. It is characterized by partial or generalized target-tissue insensitivity to glucocorticoids.
