Related Research Articles
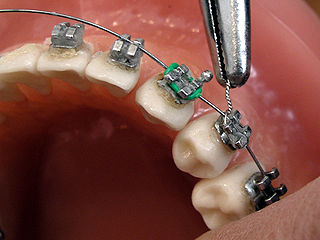
Orthodontics is a dentistry specialty that addresses the diagnosis, prevention, management, and correction of mal-positioned teeth and jaws, as well as misaligned bite patterns. It may also address the modification of facial growth, known as dentofacial orthopedics.
Hypodontia is defined as the developmental absence of one or more teeth excluding the third molars. It is one of the most common dental anomalies, and can have a negative impact on function, and also appearance. It rarely occurs in primary teeth and the most commonly affected are the adult second premolars and the upper lateral incisors. It usually occurs as part of a syndrome that involves other abnormalities and requires multidisciplinary treatment.

Prognathism, also called Habsburg chin, Habsburg's chin, Habsburg jaw or Habsburg's jaw primarily in the context of its prevalence amongst members of the House of Habsburg, is a positional relationship of the mandible or maxilla to the skeletal base where either of the jaws protrudes beyond a predetermined imaginary line in the coronal plane of the skull. In general dentistry, oral and maxillofacial surgery, and orthodontics, this is assessed clinically or radiographically (cephalometrics). The word prognathism derives from Greek πρό and γνάθος. One or more types of prognathism can result in the common condition of malocclusion, in which an individual's top teeth and lower teeth do not align properly.

In orthodontics, a malocclusion is a misalignment or incorrect relation between the teeth of the upper and lower dental arches when they approach each other as the jaws close. The English-language term dates from 1864; Edward Angle (1855–1930), the "father of modern orthodontics", popularised it. The word "malocclusion" derives from occlusion, and refers to the manner in which opposing teeth meet.
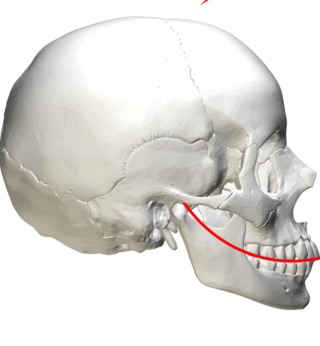
In anatomy, the Curve of Spee is defined as the curvature of the mandibular occlusal plane beginning at the canine and following the buccal cusps of the posterior teeth, continuing to the terminal molar. According to another definition the curve of Spee is an anatomic curvature of the occlusal alignment of the teeth, beginning at the tip of the lower incisor, following the buccal cusps of the natural premolars, and molars and continuing to the anterior border of the ramus. It is named for the German embryologist Ferdinand Graf von Spee (1855–1937), who was first to describe the anatomic relations of human teeth in the sagittal plane.
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.

Overjet is the extent of horizontal (anterior-posterior) overlap of the maxillary central incisors over the mandibular central incisors. In class II malocclusion the overjet is increased as the maxillary central incisors are protruded.

Crossbite is a form of malocclusion where a tooth has a more buccal or lingual position than its corresponding antagonist tooth in the upper or lower dental arch. In other words, crossbite is a lateral misalignment of the dental arches.
Serial extraction is the planned extraction of certain deciduous teeth and specific permanent teeth in an orderly sequence and predetermined pattern to guide the erupting permanent teeth into a more favorable position.
Interproximal reduction is the practice of mechanically removing enamel from between the teeth to achieve orthodontic ends, such as to correct crowding, or reshape the contact area between neighboring teeth. After reducing the enamel, the procedure should also involve anatomic re-contouring and the protection of interproximal enamel surfaces.
Dentition analyses are systems of tooth and jaw measurement used in orthodontics to understand arch space and predict any malocclusion. Example systems of dentition analysis are listed below.
Bolton Analysis is a tooth analysis developed by Wayne A. Bolton to determine the discrepancy between size of maxillary and mandibular teeth. This analysis helps to determine the optimum interarch relationship. This analysis measures the Mesio-distal width of each tooth and is divided into two analyses.
Elastics are rubber bands frequently used in the field of orthodontics to correct different types of malocclusions. The elastic wear is prescribed by an orthodontist or a dentist in an orthodontic treatment. The longevity of the elastic wear may vary from two weeks to several months. The elastic wear can be worn from 12 to 23 hours a day, either during the night or throughout the day depending on the requirements for each malocclusion. The many different types of elastics may produce different forces on teeth. Therefore, using elastics with specific forces is critical in achieving a good orthodontic occlusion.
Activator Appliance is an Orthodontics appliance that was developed by Viggo Andresen in 1908. This was one of the first functional appliances that was developed to correct functional jaw in the early 1900s. Activator appliance became the universal appliance that was used widely throughout Europe in the earlier part of the 20th century.
Frankel appliance or Frankel Functional Regulator is an orthodontic functional appliance which was developed by Rolf Fränkel in 1950s for treatment to patients of all ages. This appliance primarily focused on the modulation of neuromuscular activity in order to produce changes in jaw and teeth. The appliance was opposite to the Bionator appliance and Activator appliance.
Molar distalization is a process in the field of Orthodontics which is used to move molar teeth, especially permanent first molars, distally (backwards) in an arch. This procedure is often used in treatment of patients who have Class 2 malocclusion. The cause is often the result of loss of E space in an arch due to early loss of primary molar teeth and mesial (forward) migration of the molar teeth. Sometimes molars are distalized to make space for other impacted teeth, such as premolars or canines, in the mouth.
Intrusion is a movement in the field of orthodontics where a tooth is moved partially into the bone. Intrusion is done in orthodontics to correct an anterior deep bite or in some cases intrusion of the over-erupted posterior teeth with no opposing tooth. Intrusion can be done in many ways and consists of many different types. Intrusion, in orthodontic history, was initially defined as problematic in early 1900s and was known to cause periodontal effects such as root resorption and recession. However, in mid 1950s successful intrusion with light continuous forces was demonstrated. Charles J. Burstone defined intrusion to be "the apical movement of the geometric center of the root (centroid) in respect to the occlusal plane or plane based on the long axis of tooth".
Open bite is a type of orthodontic malocclusion which has been estimated to occur in 0.6% of the people in the United States. This type of malocclusion has no vertical overlap or contact between the anterior incisors. The term "open bite" was coined by Carevelli in 1842 as a distinct classification of malocclusion. Different authors have described the open bite in a variety of ways. Some authors have suggested that open bite often arises when overbite is less than the usual amount. Additionally, others have contended that open bite is identified by end-on incisal relationships. Lastly, some researchers have stated that a lack of incisal contact must be present to diagnose an open bite.
Orthodontic indices are one of the tools that are available for orthodontists to grade and assess malocclusion. Orthodontic indices can be useful for an epidemiologist to analyse prevalence and severity of malocclusion in any population.
References
- ↑ "The Irregularity Index: A quantitative score of mandibular anterior alignment - American Journal of Orthodontics". www.ajodo.org. Retrieved 2016-01-16.
- ↑ Bernabé, Eduardo; Flores-Mir, Carlos (2006-06-01). "Estimating arch length discrepancy through Little's Irregularity Index for epidemiological use". European Journal of Orthodontics. 28 (3): 269–273. doi: 10.1093/ejo/cji112 . ISSN 0141-5387. PMID 16648212.
- ↑ Macauley, Donal; Garvey, Thérèse M.; Dowling, Adam H.; Fleming, Garry J. P. (2012-12-01). "Using Little's Irregularity Index in orthodontics: Outdated and inaccurate?". Journal of Dentistry. 40 (12): 1127–1133. doi:10.1016/j.jdent.2012.09.010. PMID 23000526.