
Ectopic pregnancy is a complication of pregnancy in which the embryo attaches outside the uterus. Signs and symptoms classically include abdominal pain and vaginal bleeding, but fewer than 50 percent of affected women have both of these symptoms. The pain may be described as sharp, dull, or crampy. Pain may also spread to the shoulder if bleeding into the abdomen has occurred. Severe bleeding may result in a fast heart rate, fainting, or shock. With very rare exceptions, the fetus is unable to survive.

A cyst, also traditionally known from Old English as a wen, is a closed sac, having a distinct envelope and division compared with the nearby tissue. Hence, it is a cluster of cells that have grouped together to form a sac ; however, the distinguishing aspect of a cyst is that the cells forming the "shell" of such a sac are distinctly abnormal when compared with all surrounding cells for that given location. A cyst may contain air, fluids, or semi-solid material. A collection of pus is called an abscess, not a cyst. Once formed, a cyst may resolve on its own. When a cyst fails to resolve, it may need to be removed surgically, but that would depend upon its type and location.

An ovarian cyst is a fluid-filled sac within the ovary. Often they cause no symptoms. Occasionally they may produce bloating, lower abdominal pain, or lower back pain. The majority of cysts are harmless. If the cyst either breaks open or causes twisting of the ovary, it may cause severe pain. This may result in vomiting or feeling faint, and even cause head aches.
Oophorectomy, historically also called ovariotomy is the surgical removal of an ovary or ovaries. The surgery is also called ovariectomy, but this term is mostly used in reference to animals, e.g. the surgical removal of ovaries from laboratory animals. Removal of the ovaries of females is the biological equivalent of castration of males; the term castration is only occasionally used in the medical literature to refer to oophorectomy of women. In veterinary medicine, the removal of ovaries and uterus is called ovariohysterectomy (spaying) and is a form of sterilization.

Surface epithelial-stromal tumors are a class of ovarian neoplasms that may be benign or malignant. Neoplasms in this group are thought to be derived from the ovarian surface epithelium or from ectopic endometrial or fallopian tube (tubal) tissue. Tumors of this type are also called ovarian adenocarcinoma. This group of tumors accounts for 90% to 95% of all cases of ovarian cancer; however is mainly only found in postmenopausal women with the exception of the United States where 7% of cases occur in women under the age of 40. Serum CA-125 is often elevated but is only 50% accurate so it is not a useful tumor marker to assess the progress of treatment. 75% of women with epithelial ovarian cancer are found within the advanced-stages; however younger patients are more likely to have better prognoses than older patients.

Adenomyosis is a medical condition characterized by the growth of cells that proliferate on the inside of the uterus (endometrium) atypically located among the cells of the uterine wall (myometrium), as a result, thickening of the uterus occurs. As well as being misplaced in patients with this condition, endometrial tissue is completely functional. The tissue thickens, sheds and bleeds during every menstrual cycle.

Gynecologic ultrasonography or gynecologic sonography refers to the application of medical ultrasonography to the female pelvic organs as well as the bladder, the adnexa, and the recto-uterine pouch. The procedure may lead to other medically relevant findings in the pelvis.This technique is useful to detect myomas or mullerian malformations.
A hydrosalpinx is a condition that occurs when a fallopian tube is blocked and fills with serous or clear fluid near the ovary. The blocked tube may become substantially distended giving the tube a characteristic sausage-like or retort-like shape. The condition is often bilateral and the affected tubes may reach several centimeters in diameter. The blocked tubes cause infertility. A fallopian tube filled with blood is a hematosalpinx, and with pus a pyosalpinx.

The appendix testis is a vestigial remnant of the Müllerian duct, present on the upper pole of the testis and attached to the tunica vaginalis. It is present about 90% of the time and is homologous to the fallopian tubes in females.
A uterine septum is a congenital uterine malformation where the uterine cavity is partitioned by a longitudinal septum; the outside of the uterus has a normal typical shape. The wedge-like partition may involve only the superior part of the cavity resulting in an incomplete septum or a subseptate uterus, or less frequently the total length of the cavity and the cervix resulting in a double cervix. The septation may also continue caudally into the vagina resulting in a "double vagina".
Fallopian tube obstruction, also known as fallopian tube occlusion is a major cause of female infertility. Blocked fallopian tubes are unable to let the ovum and the sperm converge, thus making fertilization impossible.
An adnexal mass is a lump in the tissue of the adnexa of the uterus. Adnexal masses can be benign (noncancerous) or malignant (cancerous), and they can be categorized as simple or complex.
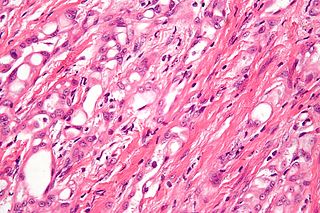
Adenomatoid tumors are rare and benign mesothelial tumors, which arise from the lining of organs. It mainly presents in the genital tract, in regions such as the testis and epididymis. Because of this, researchers had a difficult time concluding that type of tumor has a mesothelial origin. Immunohistochemistry staining of tumor samples show that it is indeed positive for mesothelial-markers. It is the most common extratesticular neoplasm after lipoma, and accounts for 30% of these masses. On the other hand, adenomatoid tumors are the most common tumors of testicular adnexa. Although they are more common to be found in the paratesticular region they are sometimes found in the intratesticular region. It also has been found in other organs such as the pancreas, liver, mesocolon, and adrenal glands. In the female, it has been found in the body of the uterus and the fallopian tube. Most adenomatoid tumors do not cause much pain and can go unnoticed for a long time. Of course, there are a few exceptions to this absence of pain. An example of this is when adenomatoid tumors grow too close to testicular adnexal structures. Tumors of this kind are usually found to be asymptomatic and easily treatable.
Primary fallopian tube cancer (PFTC), often just tubal cancer, is a malignant neoplasm that originates from the fallopian tube.

Ovarian torsion (OT) or adnexal torsion is an abnormal condition where an ovary twists on its attachment to other structures, such that blood flow is decreased. Symptoms typically include pelvic pain on one side. While classically the pain is sudden in onset, this is not always the case. Other symptoms may include nausea. Complications may include infection, bleeding, or infertility.

A corpus luteum cyst is a type of ovarian cyst which may rupture about the time of menstruation, and take up to three months to disappear entirely. A corpus luteum cyst rarely occurs in women over the age of 50, because eggs are no longer being released after menopause. Corpus luteum cysts may contain blood and other fluids. The physical shape of a corpus luteum cyst may appear as an enlargement of the ovary itself, rather than a distinct mass -like growth on the surface of the ovary.

Complete androgen insensitivity syndrome (CAIS) is an AIS condition that results in the complete inability of the cell to respond to androgens. As such, the insensitivity to androgens is only clinically significant when it occurs in individuals who are exposed to significant amounts of testosterone at some point in their lives. The unresponsiveness of the cell to the presence of androgenic hormones prevents the masculinization of male genitalia in the developing fetus, as well as the development of male secondary sexual characteristics at puberty, but does allow, without significant impairment, female genital and sexual development in those with the condition.
Theca lutein cyst is a type of bilateral functional ovarian cyst filled with clear, straw-colored fluid. These cysts result from exaggerated physiological stimulation due to elevated levels of beta-human chorionic gonadotropin (beta-hCG) or hypersensitivity to beta-hCG. On ultrasound and MRI, theca lutein cysts appear in multiples on ovaries that are enlarged.

Endosalpingiosis is a condition in which fallopian tube-like epithelium is found outside the fallopian tube. It is unknown what causes this condition. It is generally accepted that the condition develops from transformation of coelomic tissue. It is often an incidental finding and is not usually associated with any pathology.

Tubal factor infertility (TFI) is female infertility caused by diseases, obstructions, damage, scarring, congenital malformations or other factors which impede the descent of a fertilized or unfertilized ovum into the uterus through the fallopian tubes and prevents a normal pregnancy and full term birth. Tubal factors cause 25-30% of infertility cases. Tubal factor is one complication of chlamydia trachomatis infection in women.

