
Streptococcus is a genus of gram-positive coccus or spherical bacteria that belongs to the family Streptococcaceae, within the order Lactobacillales, in the phylum Firmicutes. Cell division in streptococci occurs along a single axis, so as they grow, they tend to form pairs or chains that may appear bent or twisted. This differs from staphylococci, which divide along multiple axes, thereby generating irregular, grape-like clusters of cells. Most streptococci are oxidase-negative and catalase-negative, and many are facultative anaerobes.

Pneumonia is an inflammatory condition of the lung primarily affecting the small air sacs known as alveoli. Symptoms typically include some combination of productive or dry cough, chest pain, fever, and difficulty breathing. The severity of the condition is variable.

Sputum is mucus that is coughed up from the lower airways. In medicine, sputum samples are usually used for naked eye exam, microbiological investigation of respiratory infections and cytological investigations of respiratory systems. It is crucial that the specimen not include any mucoid material from the nose.
Atypical pneumonia, also known as walking pneumonia, is any type of pneumonia not caused by one of the pathogens most commonly associated with the disease. Its clinical presentation contrasts to that of "typical" pneumonia. A variety of microorganisms can cause it. When it develops independently from another disease, it is called primary atypical pneumonia (PAP).
Mycoplasma pneumoniae is a very small bacterium in the class Mollicutes. It is a human pathogen that causes the disease mycoplasma pneumonia, a form of atypical bacterial pneumonia related to cold agglutinin disease. M. pneumoniae is characterized by the absence of a peptidoglycan cell wall and resulting resistance to many antibacterial agents. The persistence of M. pneumoniae infections even after treatment is associated with its ability to mimic host cell surface composition.
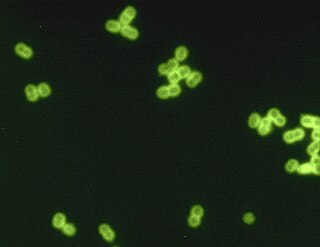
Streptococcus pneumoniae, or pneumococcus, is a Gram-positive, spherical bacteria, alpha-hemolytic or beta-hemolytic, aerotolerant anaerobic member of the genus Streptococcus. They are usually found in pairs (diplococci) and do not form spores and are non motile. As a significant human pathogenic bacterium S. pneumoniae was recognized as a major cause of pneumonia in the late 19th century, and is the subject of many humoral immunity studies.

Klebsiella pneumoniae is a Gram-negative, non-motile, encapsulated, lactose-fermenting, facultative anaerobic, rod-shaped bacterium. It appears as a mucoid lactose fermenter on MacConkey agar.

Pleural empyema is a collection of pus in the pleural cavity caused by microorganisms, usually bacteria. Often it happens in the context of a pneumonia, injury, or chest surgery. It is one of the various kinds of pleural effusion. There are three stages: exudative, when there is an increase in pleural fluid with or without the presence of pus; fibrinopurulent, when fibrous septa form localized pus pockets; and the final organizing stage, when there is scarring of the pleura membranes with possible inability of the lung to expand. Simple pleural effusions occur in up to 40% of bacterial pneumonias. They are usually small and resolve with appropriate antibiotic therapy. If however an empyema develops additional intervention is required.

Haemophilus influenzae is a Gram-negative, coccobacillary, facultatively anaerobic capnophilic pathogenic bacterium of the family Pasteurellaceae. H. influenzae was first described in 1892 by Richard Pfeiffer during an influenza pandemic. He incorrectly described Haemophilus influenzae as the causative microbe, which retains "influenza" in its name.

The bacterial capsule is a large structure common to many bacteria. It is a polysaccharide layer that lies outside the cell envelope, and is thus deemed part of the outer envelope of a bacterial cell. It is a well-organized layer, not easily washed off, and it can be the cause of various diseases.

An opportunistic infection is an infection caused by pathogens that take advantage of an opportunity not normally available. These opportunities can stem from a variety of sources, such as a weakened immune system, an altered microbiome, or breached integumentary barriers. Many of these pathogens do not cause disease in a healthy host that has a non-compromised immune system, and can, in some cases, act as commensals until the balance of the immune system is disrupted. Opportunistic infections can also be attributed to pathogens that cause mild illness in healthy individuals but lead to more serious illness when given the opportunity to take advantage of an immunocompromised host.

A diplococcus is a round bacterium that typically occurs in the form of two joined cells.
Community-acquired pneumonia (CAP) refers to pneumonia contracted by a person outside of the healthcare system. In contrast, hospital-acquired pneumonia (HAP) is seen in patients who have recently visited a hospital or who live in long-term care facilities. CAP is common, affecting people of all ages, and its symptoms occur as a result of oxygen-absorbing areas of the lung (alveoli) filling with fluid. This inhibits lung function, causing dyspnea, fever, chest pains and cough.
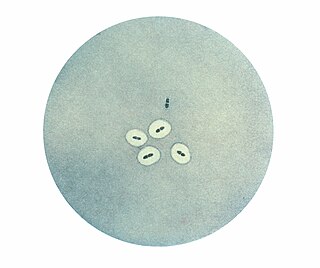
The quellung reaction, also called the Neufeld reaction, is a biochemical reaction in which antibodies bind to the bacterial capsule of Streptococcus pneumoniae, Klebsiella pneumoniae, Neisseria meningitidis, Bacillus anthracis, Haemophilus influenzae, Escherichia coli, and Salmonella. The antibody reaction allows these species to be visualized under a microscope. If the reaction is positive, the capsule becomes opaque and appears to enlarge.

Pathogenic bacteria are bacteria that can cause disease. This article focuses on the bacteria that are pathogenic to humans. Most species of bacteria are harmless and are often beneficial but others can cause infectious diseases. The number of these pathogenic species in humans is estimated to be fewer than a hundred. By contrast, several thousand species are part of the gut flora present in the digestive tract.
A pneumococcal infection is an infection caused by the bacterium Streptococcus pneumoniae, which is also called the pneumococcus. S. pneumoniae is a common member of the bacterial flora colonizing the nose and throat of 5–10% of healthy adults and 20–40% of healthy children. However, it is also a cause of significant disease, being a leading cause of pneumonia, bacterial meningitis, and sepsis. The World Health Organization estimates that in 2005 pneumococcal infections were responsible for the death of 1.6 million children worldwide.
Austrian syndrome, also known as Osler's triad, is a medical condition that was first described by Robert Austrian in 1957. The presentation of the condition consists of pneumonia, endocarditis, and meningitis, all caused by Streptococcus pneumoniae. It is associated with alcohol use disorder due to hyposplenism and can be seen in males between the ages of 40–60 years old.
Streptococcus pseudopneumoniae is a gram-positive coccus that may cause pneumonia in humans. It was first described in 2004. The organism is often mistaken for S. pneumoniae and its clinical importance is as yet uncertain. It seems likely that most cases of S. pseudopneumoniae pneumonia are misdiagnosed as S. pneumoniae.
Elaine I. Tuomanen, M.D. is an American pediatrician and chair of the Department of Infectious Diseases at St. Jude Children's Research Hospital. She is noted for her research on Molecular pathogenesis of Streptococcus pneumoniae.

Samir Kumar Saha is an eminent Bangladeshi microbiologist and public health expert. He is the professor, senior consultant and head of the department of Diagnostic Division of Microbiology at the Dhaka Shishu Hospital for children and also the executive director of The Child Health Research Foundation (CHRF) at the Bangladesh Institute of Child Health.
