In medicine, a pulse represents the tactile arterial palpation of the cardiac cycle (heartbeat) by trained fingertips. The pulse may be palpated in any place that allows an artery to be compressed near the surface of the body, such as at the neck, wrist, at the groin, behind the knee, near the ankle joint, and on foot. Pulse is equivalent to measuring the heart rate. The heart rate can also be measured by listening to the heart beat by auscultation, traditionally using a stethoscope and counting it for a minute. The radial pulse is commonly measured using three fingers. This has a reason: the finger closest to the heart is used to occlude the pulse pressure, the middle finger is used get a crude estimate of the blood pressure, and the finger most distal to the heart is used to nullify the effect of the ulnar pulse as the two arteries are connected via the palmar arches. The study of the pulse is known as sphygmology.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

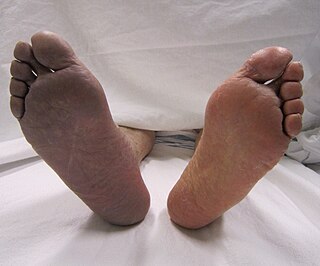
Peripheral artery disease (PAD) is an abnormal narrowing of arteries other than those that supply the heart or brain. When narrowing occurs in the heart, it is called coronary artery disease, and in the brain, it is called cerebrovascular disease. Peripheral artery disease most commonly affects the legs, but other arteries may also be involved – such as those of the arms, neck, or kidneys. The classic symptom is leg pain when walking which resolves with rest, known as intermittent claudication. Other symptoms include skin ulcers, bluish skin, cold skin, or abnormal nail and hair growth in the affected leg. Complications may include an infection or tissue death which may require amputation; coronary artery disease, or stroke. Up to 50% of people with PAD do not have symptoms.
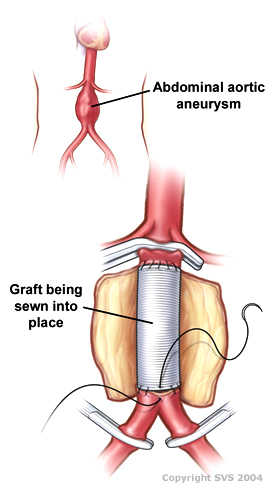
Vascular surgery is a surgical subspecialty in which vascular diseases involving the arteries, veins, or lymphatic vessels, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The specialty evolved from general and cardiovascular surgery where it refined the management of just the vessels, no longer treating the heart or other organs. Modern vascular surgery includes open surgery techniques, endovascular techniques and medical management of vascular diseases - unlike the parent specialities. The vascular surgeon is trained in the diagnosis and management of diseases affecting all parts of the vascular system excluding the coronaries and intracranial vasculature. Vascular surgeons also are called to assist other physicians to carry out surgery near vessels, or to salvage vascular injuries that include hemorrhage control, dissection, occlusion or simply for safe exposure of vascular structures.
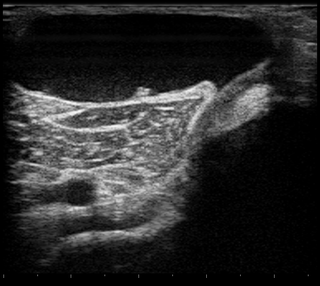
A Baker's cyst, also known as a popliteal cyst, is a type of fluid collection behind the knee. Often there are no symptoms. If symptoms do occur these may include swelling and pain behind the knee, or knee stiffness. If the cyst breaks open, pain may significantly increase with swelling of the calf. Rarely complications such as deep vein thrombosis, peripheral neuropathy, ischemia, or compartment syndrome may occur.

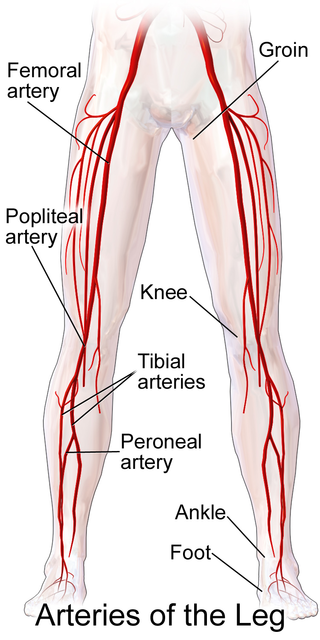
The popliteal artery is a deeply placed continuation of the femoral artery opening in the distal portion of the adductor magnus muscle. It courses through the popliteal fossa and ends at the lower border of the popliteus muscle, where it branches into the anterior and posterior tibial arteries.

In medicine, aortoiliac occlusive disease is a form of central artery disease involving the blockage of the abdominal aorta as it transitions into the common iliac arteries.

Takayasu's arteritis (TA), also known as aortic arch syndrome, nonspecific aortoarteritis, and pulseless disease, is a form of large vessel granulomatous vasculitis with massive intimal fibrosis and vascular narrowing, most commonly affecting young or middle-aged women of Asian descent, though anyone can be affected. It mainly affects the aorta and its branches, as well as the pulmonary arteries. Females are about 8–9 times more likely to be affected than males.

Arteritis is the inflammation of the walls of arteries, usually as a result of infection or autoimmune response. Arteritis, a complex disorder, is still not entirely understood. Arteritis may be distinguished by its different types, based on the organ systems affected by the disease. A complication of arteritis is thrombosis, which can be fatal. Arteritis and phlebitis are forms of vasculitis.
Intermittent claudication, also known as vascular claudication, is a symptom that describes muscle pain on mild exertion, classically in the calf muscle, which occurs during exercise, such as walking, and is relieved by a short period of rest. It is classically associated with early-stage peripheral artery disease, and can progress to critical limb ischemia unless treated or risk factors are modified and maintained.

A shin splint, also known as medial tibial stress syndrome, is pain along the inside edge of the shinbone (tibia) due to inflammation of tissue in the area. Generally this is between the middle of the lower leg and the ankle. The pain may be dull or sharp, and is generally brought on by high-impact exercise that overloads the tibia. It generally resolves during periods of rest. Complications may include stress fractures.
Claudication is a medical term usually referring to impairment in walking, or pain, discomfort, numbness, or tiredness in the legs that occurs during walking or standing and is relieved by rest. The perceived level of pain from claudication can be mild to extremely severe. Claudication is most common in the calves but it can also affect the feet, thighs, hips, buttocks, or arms. The word claudication comes from the Latin claudicare meaning 'to limp'.

The popliteal vein is a vein of the lower limb. It is formed from the anterior tibial vein and the posterior tibial vein. It travels medial to the popliteal artery, and becomes the femoral vein. It drains blood from the leg. It can be assessed using medical ultrasound. It can be affected by popliteal vein entrapment.

The plantaris is one of the superficial muscles of the superficial posterior compartment of the leg, one of the fascial compartments of the leg.
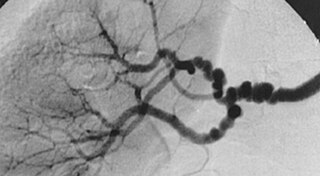
Fibromuscular dysplasia (FMD) is a non-atherosclerotic, non-inflammatory disease of the blood vessels that causes abnormal growth within the wall of an artery. FMD has been found in nearly every arterial bed in the body although the most common arteries affected are the renal and carotid arteries.
Acute limb ischaemia (ALI) occurs when there is a sudden lack of blood flow to a limb.

A knee dislocation is an injury in which there is disruption of the knee joint between the tibia and the femur. Symptoms include pain and instability of the knee. Complications may include injury to an artery, most commonly the popliteal artery behind the knee, or compartment syndrome.
Popliteal bypass surgery, more commonly known as femoropopliteal bypass or more generally as lower extremity bypass surgery, is a surgical procedure used to treat diseased leg arteries above or below the knee. It is used as a medical intervention to salvage limbs that are at risk of amputation and to improve walking ability in people with severe intermittent claudication and ischemic rest pain.
Adventitial cystic disease is a rare type of non-atherosclerotic peripheral artery disease. It can present as claudication, critical limb ischemia or acute limb ischemia. The most commonly affected vessel is the popliteal artery. The cause is unknown.

Arterial occlusion is a condition involving partial or complete blockage of blood flow through an artery. Arteries are blood vessels that carry oxygenated blood to body tissues. An occlusion of arteries disrupts oxygen and blood supply to tissues, leading to ischemia. Depending on the extent of ischemia, symptoms of arterial occlusion range from simple soreness and pain that can be relieved with rest, to a lack of sensation or paralysis that could require amputation.

