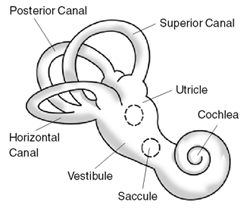
The inner ear is the innermost part of the vertebrate ear. In vertebrates, the inner ear is mainly responsible for sound detection and balance. In mammals, it consists of the bony labyrinth, a hollow cavity in the temporal bone of the skull with a system of passages comprising two main functional parts:

The sense of balance or equilibrioception is the perception of balance and spatial orientation. It helps prevent humans and nonhuman animals from falling over when standing or moving. Equilibrioception is the result of a number of sensory systems working together; the eyes, the inner ears, and the body's sense of where it is in space (proprioception) ideally need to be intact.
A balance disorder is a disturbance that causes an individual to feel unsteady, for example when standing or walking. It may be accompanied by feelings of giddiness, or wooziness, or having a sensation of movement, spinning, or floating. Balance is the result of several body systems working together: the visual system (eyes), vestibular system (ears) and proprioception. Degeneration or loss of function in any of these systems can lead to balance deficits.
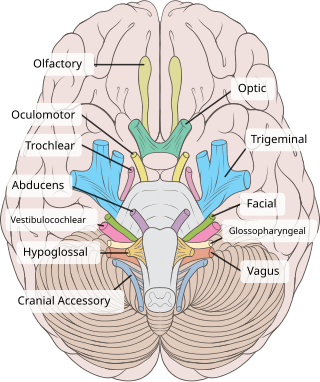
The vestibulocochlear nerve or auditory vestibular nerve, also known as the eighth cranial nerve, cranial nerve VIII, or simply CN VIII, is a cranial nerve that transmits sound and equilibrium (balance) information from the inner ear to the brain. Through olivocochlear fibers, it also transmits motor and modulatory information from the superior olivary complex in the brainstem to the cochlea.

The vestibulo-ocular reflex (VOR) is a reflex that acts to stabilize gaze during head movement, with eye movement due to activation of the vestibular system, it is also known as the Cervico-ocular reflex. The reflex acts to stabilize images on the retinas of the eye during head movement. Gaze is held steadily on a location by producing eye movements in the direction opposite that of head movement. For example, when the head moves to the right, the eyes move to the left, meaning the image a person sees stays the same even though the head has turned. Since slight head movement is present all the time, VOR is necessary for stabilizing vision: people with an impaired reflex find it difficult to read using print, because the eyes do not stabilise during small head tremors, and also because damage to reflex can cause nystagmus.

The utricle and saccule are the two otolith organs in the vertebrate inner ear. The word utricle comes from Latin uter 'leather bag'. The utricle and saccule are part of the balancing system in the vestibule of the bony labyrinth. They use small stones and a viscous fluid to stimulate hair cells to detect motion and orientation. The utricle detects linear accelerations and head-tilts in the horizontal plane.

The vestibular system, in vertebrates, is a sensory system that creates the sense of balance and spatial orientation for the purpose of coordinating movement with balance. Together with the cochlea, a part of the auditory system, it constitutes the labyrinth of the inner ear in most mammals.

Labyrinthitis is inflammation of the labyrinth, a maze of fluid-filled channels in the inner ear. Vestibular neuritis is inflammation of the vestibular nerve. Both conditions involve inflammation of the inner ear. Labyrinths that house the vestibular system sense changes in the head's position or the head's motion. Inflammation of these inner ear parts results in a vertigo and also possible hearing loss or tinnitus. It can occur as a single attack, a series of attacks, or a persistent condition that diminishes over three to six weeks. It may be associated with nausea, vomiting, and eye nystagmus.
Benign paroxysmal positional vertigo (BPPV) is a disorder arising from a problem in the inner ear. Symptoms are repeated, brief periods of vertigo with movement, characterized by a spinning sensation upon changes in the position of the head. This can occur with turning in bed or changing position. Each episode of vertigo typically lasts less than one minute. Nausea is commonly associated. BPPV is one of the most common causes of vertigo.

Electronystagmography (ENG) is a diagnostic test to record involuntary movements of the eye caused by a condition known as nystagmus. It can also be used to diagnose the cause of vertigo, dizziness or balance dysfunction by testing the vestibular system. Electronystagmography is used to assess voluntary and involuntary eye movements. It evaluates the cochlear nerve and the oculomotor nerve. The ENG can be used to determine the origin of various eye and ear disorders.

Vertigo is a condition in which a person has the sensation that they are moving, or that objects around them are moving, when they are not. Often it feels like a spinning or swaying movement. It may be associated with nausea, vomiting, perspiration, or difficulties walking. It is typically worse when the head is moved. Vertigo is the most common type of dizziness.

The vestibular nerve is one of the two branches of the vestibulocochlear nerve. In humans the vestibular nerve transmits sensory information transmitted by vestibular hair cells located in the two otolith organs and the three semicircular canals via the vestibular ganglion of Scarpa. Information from the otolith organs reflects gravity and linear accelerations of the head. Information from the semicircular canals reflects rotational movement of the head. Both are necessary for the sensation of body position and gaze stability in relation to a moving environment.

In medicine, the caloric reflex test is a test of the vestibulo-ocular reflex that involves irrigating cold or warm water or air into the external auditory canal. This method was developed by Robert Bárány, who won a Nobel prize in 1914 for this discovery.

The vestibulospinal tract is a neural tract in the central nervous system. Specifically, it is a component of the extrapyramidal system and is classified as a component of the medial pathway. Like other descending motor pathways, the vestibulospinal fibers of the tract relay information from nuclei to motor neurons. The vestibular nuclei receive information through the vestibulocochlear nerve about changes in the orientation of the head. The nuclei relay motor commands through the vestibulospinal tract. The function of these motor commands is to alter muscle tone, extend, and change the position of the limbs and head with the goal of supporting posture and maintaining balance of the body and head.
The ampullary cupula, or cupula, is a structure in the vestibular system, providing the sense of spatial orientation.
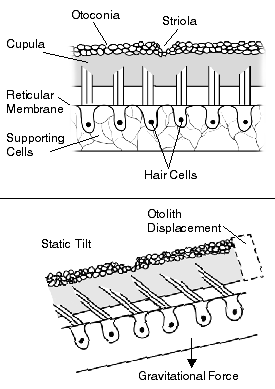
The otolithic membrane is a fibrous structure located in the vestibular system of the inner ear. It plays a critical role in the brain's interpretation of equilibrium. The membrane serves to determine if the body or the head is tilted, in addition to the linear acceleration of the body. The linear acceleration could be in the horizontal direction as in a moving car or vertical acceleration such as that felt when an elevator moves up or down.
The Epley maneuver or repositioning maneuver is a maneuver used by medical professionals to treat one common cause of vertigo, benign paroxysmal positional vertigo (BPPV) of the posterior or anterior canals of the ear. The maneuver works by allowing free-floating particles, displaced otoconia, from the affected semicircular canal to be relocated by using gravity, back into the utricle, where they can no longer stimulate the cupula, therefore relieving the patient of bothersome vertigo. The maneuver was developed by the physician John M. Epley, and was first described in 1980.
The vestibular evoked myogenic potential is a neurophysiological assessment technique used to determine the function of the otolithic organs of the inner ear. It complements the information provided by caloric testing and other forms of inner ear testing. There are two different types of VEMPs. One is the oVEMP and another is the cVEMP. The oVEMP measures integrity of the utricule and superior vestibular nerve and the cVemp measures the saccule and the inferior vestibular nerve.
Space neuroscience or astroneuroscience is the scientific study of the central nervous system (CNS) functions during spaceflight. Living systems can integrate the inputs from the senses to navigate in their environment and to coordinate posture, locomotion, and eye movements. Gravity has a fundamental role in controlling these functions. In weightlessness during spaceflight, integrating the sensory inputs and coordinating motor responses is harder to do because gravity is no longer sensed during free-fall. For example, the otolith organs of the vestibular system no longer signal head tilt relative to gravity when standing. However, they can still sense head translation during body motion. Ambiguities and changes in how the gravitational input is processed can lead to potential errors in perception, which affects spatial orientation and mental representation. Dysfunctions of the vestibular system are common during and immediately after spaceflight, such as space motion sickness in orbit and balance disorders after return to Earth.

Vestibular rehabilitation (VR), also known as vestibular rehabilitation therapy (VRT), is a specialized form of physical therapy used to treat vestibular disorders or symptoms, characterized by dizziness, vertigo, imbalance, posture, and vision. These primary symptoms can result in secondary symptoms such as nausea, fatigue, and difficulty concentrating. Symptoms of vestibular dysfunction can significantly decrease quality of life, introducing mental-emotional issues such as anxiety and depression, and greatly impair an individual, causing them to become more sedentary. Decreased mobility can result in weaker muscles, less flexible joints, and worsened stamina, as well as decreased social and occupational activity. Vestibular rehabilitation therapy can be used in conjunction with cognitive behavioral therapy in order to reduce anxiety and depression resulting from a change in lifestyle.