
A sleep disorder, or somnipathy, is a medical disorder of an individual's sleep patterns. Some sleep disorders are severe enough to interfere with normal physical, mental, social and emotional functioning. Sleep disorders are frequent and can have serious consequences on patients' health and quality of life. Polysomnography and actigraphy are tests commonly ordered for diagnosing sleep disorders.

Insomnia, also known as sleeplessness, is a sleep disorder where people have trouble sleeping. They may have difficulty falling asleep, or staying asleep for as long as desired. Insomnia is typically followed by daytime sleepiness, low energy, irritability, and a depressed mood. It may result in an increased risk of accidents of all kinds as well as problems focusing and learning. Insomnia can be short term, lasting for days or weeks, or long term, lasting more than a month. The concept of the word insomnia has two possibilities: insomnia disorder (ID) and insomnia symptoms, and many abstracts of randomized controlled trials and systematic reviews often underreport on which of these two possibilities the word insomnia refers to.

Neurotrauma, brain damage or brain injury (BI) is the destruction or degeneration of brain cells. Brain injuries occur due to a wide range of internal and external factors. In general, brain damage refers to significant, undiscriminating trauma-induced damage.
Somnolence is a state of strong desire for sleep, or sleeping for unusually long periods. It has distinct meanings and causes. It can refer to the usual state preceding falling asleep, the condition of being in a drowsy state due to circadian rhythm disorders, or a symptom of other health problems. It can be accompanied by lethargy, weakness and lack of mental agility.
Hypersomnia is a neurological disorder of excessive time spent sleeping or excessive sleepiness. It can have many possible causes and can cause distress and problems with functioning. In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), hypersomnolence, of which there are several subtypes, appears under sleep-wake disorders.
Upper airway resistance syndrome (UARS) is a sleep disorder characterized by the narrowing of the airway that can cause disruptions to sleep. The symptoms include unrefreshing sleep, fatigue, sleepiness, chronic insomnia, and difficulty concentrating. UARS can be diagnosed by polysomnograms capable of detecting Respiratory Effort-related Arousals. It can be treated with lifestyle changes, functional orthodontics, surgery, mandibular repositioning devices or CPAP therapy. UARS is considered a variant of sleep apnea, although some scientists and doctors believe it to be a distinct disorder.
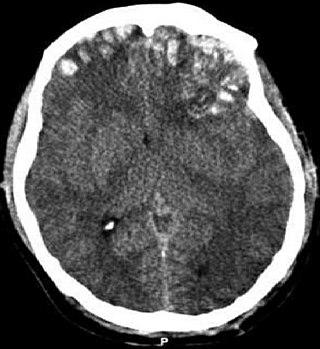
A traumatic brain injury (TBI), also known as an intracranial injury, is an injury to the brain caused by an external force. TBI can be classified based on severity ranging from mild traumatic brain injury (mTBI/concussion) to severe traumatic brain injury. TBI can also be characterized based on mechanism or other features. Head injury is a broader category that may involve damage to other structures such as the scalp and skull. TBI can result in physical, cognitive, social, emotional and behavioral symptoms, and outcomes can range from complete recovery to permanent disability or death.

Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder and is characterized by recurrent episodes of complete or partial obstruction of the upper airway leading to reduced or absent breathing during sleep. These episodes are termed "apneas" with complete or near-complete cessation of breathing, or "hypopneas" when the reduction in breathing is partial. In either case, a fall in blood oxygen saturation, a disruption in sleep, or both, may result. A high frequency of apneas or hypopneas during sleep may interfere with the quality of sleep, which – in combination with disturbances in blood oxygenation – is thought to contribute to negative consequences to health and quality of life. The terms obstructive sleep apnea syndrome (OSAS) or obstructive sleep apnea–hypopnea syndrome (OSAHS) may be used to refer to OSA when it is associated with symptoms during the daytime.
Post-concussion syndrome (PCS), also known as persisting symptoms after concussion, is a set of symptoms that may continue for weeks, months, or years after a concussion. PCS is medically classified as a mild traumatic brain injury (TBI). About 35% of people with concussion experience persistent or prolonged symptoms 3 to 6 months after injury. Prolonged concussion is defined as having concussion symptoms for over four weeks following the first accident in youth and for weeks or months in adults.
The International Classification of Sleep Disorders (ICSD) is "a primary diagnostic, epidemiological and coding resource for clinicians and researchers in the field of sleep and sleep medicine". The ICSD was produced by the American Academy of Sleep Medicine (AASM) in association with the European Sleep Research Society, the Japanese Society of Sleep Research, and the Latin American Sleep Society. The classification was developed as a revision and update of the Diagnostic Classification of Sleep and Arousal Disorders (DCSAD) that was produced by both the Association of Sleep Disorders Centers (ASDC) and the Association for the Psychophysiological Study of Sleep and was published in the journal Sleep in 1979. A second edition, called ICSD-2, was published by the AASM in 2005. The third edition, ICSD-3, was released by the AASM in 2014. A text revision of the third edition (ICSD-3-TR) was published in 2023 by the AASM.

Sleep medicine is a medical specialty or subspecialty devoted to the diagnosis and therapy of sleep disturbances and disorders. From the middle of the 20th century, research has provided increasing knowledge of, and answered many questions about, sleep–wake functioning. The rapidly evolving field has become a recognized medical subspecialty in some countries. Dental sleep medicine also qualifies for board certification in some countries. Properly organized, minimum 12-month, postgraduate training programs are still being defined in the United States. In some countries, the sleep researchers and the physicians who treat patients may be the same people.

Sleep deprivation, also known as sleep insufficiency or sleeplessness, is the condition of not having adequate duration and/or quality of sleep to support decent alertness, performance, and health. It can be either chronic or acute and may vary widely in severity. All known animals sleep or exhibit some form of sleep behavior, and the importance of sleep is self-evident for humans, as nearly a third of a person's life is spent sleeping.
Traumatic brain injury can cause a variety of complications, health effects that are not TBI themselves but that result from it. The risk of complications increases with the severity of the trauma; however even mild traumatic brain injury can result in disabilities that interfere with social interactions, employment, and everyday living. TBI can cause a variety of problems including physical, cognitive, emotional, and behavioral complications.
Idiopathic hypersomnia(IH) is a neurological disorder which is characterized primarily by excessive sleep and excessive daytime sleepiness (EDS). Idiopathic hypersomnia was first described by Bedrich Roth in 1976, and it can be divided into two forms: polysymptomatic and monosymptomatic. The condition typically becomes evident in early adulthood and most patients diagnosed with IH will have had the disorder for many years prior to their diagnosis. As of August 2021, an FDA-approved medication exists for IH called Xywav, which is oral solution of calcium, magnesium, potassium, and sodium oxybates; in addition to several off-label treatments (primarily FDA-approved narcolepsy medications).
Irregular sleep–wake rhythm disorder (ISWRD) is a rare form of circadian rhythm sleep disorder. It is characterized by numerous naps throughout the 24-hour period, no main nighttime sleep episode, and irregularity from day to day. Affected individuals have no pattern of when they are awake or asleep, may have poor quality sleep, and often may be very sleepy while they are awake. The total time asleep per 24 hours is normal for the person's age. The disorder is serious—an invisible disability. It can create social, familial, and work problems, making it hard for a person to maintain relationships and responsibilities, and may make a person home-bound and isolated.
An orexin receptor antagonist, or orexin antagonist, is a drug that inhibits the effect of orexin by acting as a receptor antagonist of one (selective orexin receptor antagonist or SORA) or both (dual orexin receptor antagonis or DORA) of the orexin receptors, OX1 and OX2. Medical applications include treatment of sleep disorders such as insomnia.

TIK-301 (LY-156735) is an agonist for the melatonin receptors MT1 and MT2 that is under development for the treatment of insomnia and other sleep disorders. Its agonist action on MT1 and MT2 receptors in the suprachiasmatic nucleus in the brain enables its action as a chronobiotic. It is in the same class of melatonin receptor agonists as ramelteon and tasimelteon.
Sleep is known to play an important role in the etiology and maintenance of bipolar disorder. Patients with bipolar disorder often have a less stable and more variable circadian activity. Circadian activity disruption can be apparent even if the person concerned is not currently ill.

Behavioral sleep medicine (BSM) is a field within sleep medicine that encompasses scientific inquiry and clinical treatment of sleep-related disorders, with a focus on the psychological, physiological, behavioral, cognitive, social, and cultural factors that affect sleep, as well as the impact of sleep on those factors. The clinical practice of BSM is an evidence-based behavioral health discipline that uses primarily non-pharmacological treatments. BSM interventions are typically problem-focused and oriented towards specific sleep complaints, but can be integrated with other medical or mental health treatments. The primary techniques used in BSM interventions involve education and systematic changes to the behaviors, thoughts, and environmental factors that initiate and maintain sleep-related difficulties.
Sleep epigenetics is the field of how epigenetics affects sleep.
