
Breast cancer is a cancer that develops from breast tissue. Signs of breast cancer may include a lump in the breast, a change in breast shape, dimpling of the skin, milk rejection, fluid coming from the nipple, a newly inverted nipple, or a red or scaly patch of skin. In those with distant spread of the disease, there may be bone pain, swollen lymph nodes, shortness of breath, or yellow skin.

Cancer is a group of diseases involving abnormal cell growth with the potential to invade or spread to other parts of the body. These contrast with benign tumors, which do not spread. Possible signs and symptoms include a lump, abnormal bleeding, prolonged cough, unexplained weight loss, and a change in bowel movements. While these symptoms may indicate cancer, they can also have other causes. Over 100 types of cancers affect humans.

Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum. Signs and symptoms may include blood in the stool, a change in bowel movements, weight loss, abdominal pain and fatigue. Most colorectal cancers are due to old age and lifestyle factors, with only a small number of cases due to underlying genetic disorders. Risk factors include diet, obesity, smoking, and lack of physical activity. Dietary factors that increase the risk include red meat, processed meat, and alcohol. Another risk factor is inflammatory bowel disease, which includes Crohn's disease and ulcerative colitis. Some of the inherited genetic disorders that can cause colorectal cancer include familial adenomatous polyposis and hereditary non-polyposis colon cancer; however, these represent less than 5% of cases. It typically starts as a benign tumor, often in the form of a polyp, which over time becomes cancerous.

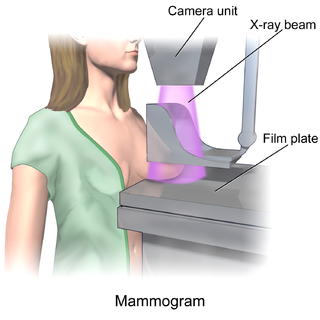
Mammography is the process of using low-energy X-rays to examine the human breast for diagnosis and screening. The goal of mammography is the early detection of breast cancer, typically through detection of characteristic masses or microcalcifications.

Prostate-specific antigen (PSA), also known as gamma-seminoprotein or kallikrein-3 (KLK3), P-30 antigen, is a glycoprotein enzyme encoded in humans by the KLK3 gene. PSA is a member of the kallikrein-related peptidase family and is secreted by the epithelial cells of the prostate gland in men and the paraurethral glands in women.

Digital rectal examination (DRE), also known as a prostate exam, is an internal examination of the rectum performed by a healthcare provider.

In a physical examination, medical examination, clinical examination, or medical checkup, a medical practitioner examines a patient for any possible medical signs or symptoms of a medical condition. It generally consists of a series of questions about the patient's medical history followed by an examination based on the reported symptoms. Together, the medical history and the physical examination help to determine a diagnosis and devise the treatment plan. These data then become part of the medical record.

Screening, in medicine, is a strategy used to look for as-yet-unrecognised conditions or risk markers. This testing can be applied to individuals or to a whole population without symptoms or signs of the disease being screened.
Overdiagnosis is the diagnosis of disease that will never cause symptoms or death during a patient's ordinarily expected lifetime and thus presents no practical threat regardless of being pathologic. Overdiagnosis is a side effect of screening for early forms of disease. Although screening saves lives in some cases, in others it may turn people into patients unnecessarily and may lead to treatments that do no good and perhaps do harm. Given the tremendous variability that is normal in biology, it is inherent that the more one screens, the more incidental findings will generally be found. For a large percentage of them, the most appropriate medical response is to recognize them as something that does not require intervention; but determining which action a particular finding warrants can be very difficult, whether because the differential diagnosis is uncertain or because the risk ratio is uncertain.
Prostate cancer screening is the screening process used to detect undiagnosed prostate cancer in men without signs or symptoms. When abnormal prostate tissue or cancer is found early, it may be easier to treat and cure, but it is unclear if early detection reduces mortality rates.

Lung cancer screening refers to cancer screening strategies used to identify early lung cancers before they cause symptoms, at a point where they are more likely to be curable. Lung cancer screening is critically important because of the incidence and prevalence of lung cancer. More than 235,000 new cases of lung cancer are expected in the United States in 2021 with approximately 130,000 deaths expected in 2021. In addition, at the time of diagnosis, 57% of lung cancers are discovered in advanced stages, meaning they are more widespread or aggressive cancers. Because there is a substantially higher probability of long-term survival following treatment of localized (60%) versus advanced stage (6%) lung cancer, lung cancer screening aims to diagnose the disease in the localized stage.
The United States Preventive Services Task Force (USPSTF) is "an independent panel of experts in primary care and prevention that systematically reviews the evidence of effectiveness and develops recommendations for clinical preventive services". The task force, a volunteer panel of primary care clinicians with methodology experience including epidemiology, biostatistics, health services research, decision sciences, and health economics, is funded, staffed, and appointed by the U.S. Department of Health and Human Services' Agency for Healthcare Research and Quality.
Breast cancer screening is the medical screening of asymptomatic, apparently healthy women for breast cancer in an attempt to achieve an earlier diagnosis. The assumption is that early detection will improve outcomes. A number of screening tests have been employed, including clinical and self breast exams, mammography, genetic screening, ultrasound, and magnetic resonance imaging.

Molecular breast imaging (MBI), also known as scintimammography, is a type of breast imaging test that is used to detect cancer cells in breast tissue of individuals who have had abnormal mammograms, especially for those who have dense breast tissue, post-operative scar tissue or breast implants.

Cervical cancer screening is a medical screening test designed to identify risk of cervical cancer. Cervical screening may involve looking for viral DNA, and/or to identify abnormal, potentially precancerous cells within the cervix as well as cells that have progressed to early stages of cervical cancer. One goal of cervical screening is to allow for intervention and treatment so abnormal lesions can be removed prior to progression to cancer. An additional goal is to decrease mortality from cervical cancer by identifying cancerous lesions in their early stages and providing treatment prior to progression to more invasive disease.

Positron emission mammography (PEM) is a nuclear medicine imaging modality used to detect or characterise breast cancer. Mammography typically refers to x-ray imaging of the breast, while PEM uses an injected positron emitting isotope and a dedicated scanner to locate breast tumors. Scintimammography is another nuclear medicine breast imaging technique, however it is performed using a gamma camera. Breasts can be imaged on standard whole-body PET scanners, however dedicated PEM scanners offer advantages including improved resolution.
Dynamic angiothermography (DATG) is a technique for the diagnosis of breast cancer. This technique, though springing from the previous conception of thermography, is based on a completely different principle. DATG records the temperature variations linked to the vascular changes in the breast due to angiogenesis. The presence, change, and growth of tumors and lesions in breast tissue change the vascular network in the breast. Consequently, through measuring the vascular structure over time, DATG effectively monitors the change in breast tissue due to tumors and lesions. It is currently used in combination with other techniques for diagnosis of breast cancer. This diagnostic method is a low-cost one compared with other techniques.
Overscreening, also called unnecessary screening, is the performance of medical screening without a medical indication to do so. Screening is a medical test in a healthy person who is showing no symptoms of a disease and is intended to detect a disease so that a person may prepare to respond to it. Screening is indicated in people who have some threshold risk for getting a disease, but is not indicated in people who are unlikely to develop a disease. Overscreening is a type of unnecessary health care.
Cancer prevention is the practice of taking active measures to decrease the incidence of cancer and mortality. The practice of prevention is dependent upon both individual efforts to improve lifestyle and seek preventive screening, and socioeconomic or public policy related to cancer prevention. Globalized cancer prevention is regarded as a critical objective due to its applicability to large populations, reducing long term effects of cancer by promoting proactive health practices and behaviors, and its perceived cost-effectiveness and viability for all socioeconomic classes.
In medicine, breast imaging is a sub-speciality of diagnostic radiology that involves imaging of the breasts for screening or diagnostic purposes. There are various methods of breast imaging using a variety of technologies as described in detail below. Traditional screening and diagnostic mammography uses x-ray technology and has been the mainstay of breast imaging for many decades. Breast tomosynthesis is a relatively new digital x-ray mammography technique that produces multiple image slices of the breast similar to, but distinct from, computed tomography (CT). Xeromammography and galactography are somewhat outdated technologies that also use x-ray technology and are now used infrequently in the detection of breast cancer. Breast ultrasound is another technology employed in diagnosis and screening that can help differentiate between fluid filled and solid lesions, an important factor to determine if a lesion may be cancerous. Breast MRI is a technology typically reserved for high-risk patients and patients recently diagnosed with breast cancer. Lastly, scintimammography is used in a subgroup of patients who have abnormal mammograms or whose screening is not reliable on the basis of using traditional mammography or ultrasound.


