
Fructose, or fruit sugar, is a ketonic simple sugar found in many plants, where it is often bonded to glucose to form the disaccharide sucrose. It is one of the three dietary monosaccharides, along with glucose and galactose, that are absorbed directly into blood during digestion. Fructose was discovered by French chemist Augustin-Pierre Dubrunfaut in 1847. The name "fructose" was coined in 1857 by the English chemist William Allen Miller. Pure, dry fructose is a sweet, white, odorless, crystalline solid, and is the most water-soluble of all the sugars. Fructose is found in honey, tree and vine fruits, flowers, berries, and most root vegetables.
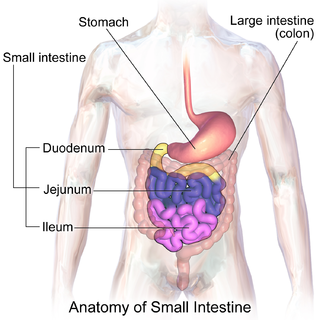
The small intestine or small bowel is an organ in the gastrointestinal tract where most of the absorption of nutrients from food takes place. It lies between the stomach and large intestine, and receives bile and pancreatic juice through the pancreatic duct to aid in digestion. The small intestine is about 18 feet long and folds many times to fit in the abdomen. Although it is longer than the large intestine, it is called the small intestine because it is narrower in width.
In cellular biology, active transport is the movement of molecules across a cell membrane from a region of lower concentration to a region of higher concentration—against the concentration gradient. Active transport requires cellular energy to achieve this movement. There are two types of active transport: primary active transport that uses adenosine triphosphate (ATP), and secondary active transport that uses an electrochemical gradient.

Digestion is the breakdown of large insoluble food molecules into small water-soluble food molecules so that they can be absorbed into the watery blood plasma. In certain organisms, these smaller substances are absorbed through the small intestine into the blood stream. Digestion is a form of catabolism that is often divided into two processes based on how food is broken down: mechanical and chemical digestion. The term mechanical digestion refers to the physical breakdown of large pieces of food into smaller pieces which can subsequently be accessed by digestive enzymes. Mechanical digestion takes place in mouth through mastication and in small intestine through segmentation contractions. In chemical digestion, enzymes break down food into the small molecules the body can use.
Carbohydrate metabolism is the whole of the biochemical processes responsible for the metabolic formation, breakdown, and interconversion of carbohydrates in living organisms.

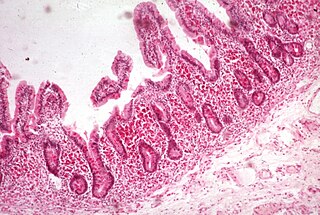
Enterocytes, or intestinal absorptive cells, are simple columnar epithelial cells which line the inner surface of the small and large intestines. A glycocalyx surface coat contains digestive enzymes. Microvilli on the apical surface increase its surface area. This facilitates transport of numerous small molecules into the enterocyte from the intestinal lumen. These include broken down proteins, fats, and sugars, as well as water, electrolytes, vitamins, and bile salts. Enterocytes also have an endocrine role, secreting hormones such as leptin.
Malabsorption is a state arising from abnormality in absorption of food nutrients across the gastrointestinal (GI) tract. Impairment can be of single or multiple nutrients depending on the abnormality. This may lead to malnutrition and a variety of anaemias.
Digestive enzymes are a group of enzymes that break down polymeric macromolecules into their smaller building blocks, in order to facilitate their absorption by the body. Digestive enzymes are found in the digestive tracts of animals and in the tracts of carnivorous plants, where they aid in the digestion of food, as well as inside cells, especially in their lysosomes, where they function to maintain cellular survival. Digestive enzymes of diverse specificities are found in the saliva secreted by the salivary glands, in the secretions of cells lining the stomach, in the pancreatic juice secreted by pancreatic exocrine cells, and in the secretions of cells lining the small and large intestines.
Sucrase is a digestive enzyme that catalyzes the hydrolysis of sucrose to its subunits fructose and glucose. One form, sucrase-isomaltase, is secreted in the small intestine on the brush border. The sucrase enzyme invertase, which occurs more commonly in plants, also hydrolyzes sucrose but by a different mechanism.

Glucose transporters are a wide group of membrane proteins that facilitate the transport of glucose across the plasma membrane, a process known as facilitated diffusion. Because glucose is a vital source of energy for all life, these transporters are present in all phyla. The GLUT or SLC2A family are a protein family that is found in most mammalian cells. 14 GLUTS are encoded by human genome. GLUT is a type of uniporter transporter protein.
Disaccharidases are glycoside hydrolases, enzymes that break down certain types of sugars called disaccharides into simpler sugars called monosaccharides. In the human body, disaccharidases are made mostly in an area of the small intestine's wall called the brush border, making them members of the group of "brush border enzymes".
Sodium-dependent glucose cotransporters are a family of glucose transporter found in the intestinal mucosa (enterocytes) of the small intestine (SGLT1) and the proximal tubule of the nephron. They contribute to renal glucose reabsorption. In the kidneys, 100% of the filtered glucose in the glomerulus has to be reabsorbed along the nephron. If the plasma glucose concentration is too high (hyperglycemia), glucose passes into the urine (glucosuria) because SGLT are saturated with the filtered glucose.
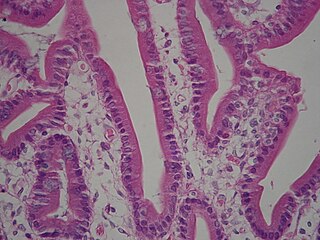
A brush border is the microvilli-covered surface of simple cuboidal and simple columnar epithelium found in different parts of the body. Microvilli are approximately 100 nanometers in diameter and their length varies from approximately 100 to 2,000 nanometers in length. Because individual microvilli are so small and are tightly packed in the brush border, individual microvilli can only be resolved using electron microscopes; with a light microscope they can usually only be seen collectively as a fuzzy fringe at the surface of the epithelium. This fuzzy appearance gave rise to the term brush border, as early anatomists noted that this structure appeared very much like the bristles of a paintbrush.

Sucrose intolerance or genetic sucrase-isomaltase deficiency (GSID) is the condition in which sucrase-isomaltase, an enzyme needed for proper metabolism of sucrose (sugar) and starch, is not produced or the enzyme produced is either partially functional or non-functional in the small intestine. All GSID patients lack fully functional sucrase, while the isomaltase activity can vary from minimal functionality to almost normal activity. The presence of residual isomaltase activity may explain why some GSID patients are better able to tolerate starch in their diet than others with GSID.
Renal glycosuria is a rare condition in which the simple sugar glucose is excreted in the urine despite normal or low blood glucose levels. With normal kidney (renal) function, glucose is excreted in the urine only when there are abnormally elevated levels of glucose in the blood. However, in those with renal glycosuria, glucose is abnormally elevated in the urine due to improper functioning of the renal tubules, which are primary components of nephrons, the filtering units of the kidneys.

Sodium/glucose cotransporter 1 (SGLT1) also known as solute carrier family 5 member 1 is a protein in humans that is encoded by the SLC5A1 gene which encodes the production of the SGLT1 protein to line the absorptive cells in the small intestine and the epithelial cells of the kidney tubules of the nephron for the purpose of glucose uptake into cells. Through the use of the sodium glucose cotransporter 1 protein, cells are able to obtain glucose which is further utilized to make and store energy for the cell.
Inborn errors of carbohydrate metabolism are inborn error of metabolism that affect the catabolism and anabolism of carbohydrates.
Iminoglycinuria, is an autosomal recessive disorder of renal tubular transport affecting reabsorption of the amino acid glycine, and the imino acids proline and hydroxyproline. This results in excess urinary excretion of all three acids.

Robert Kellogg Crane was an American biochemist best known for his discovery of sodium-glucose cotransport.
Chronic diarrheaof infancy, also called toddler's diarrhea, is a common condition typically affecting up to 1.7 billion children between ages 6–30 months worldwide every year, usually resolving by age 4. According to the World Health Organization (WHO), diarrheal disease is the second greatest cause of death in children 5 years and younger. Diarrheal disease takes the lives of 525,000 or more children per year. Diarrhea is characterized as the condition of passing of three or more loose or watery bowel movements within a day sometimes with undigested food visible. Diarrhea is separated into three clinical categories; acute diarrhea may last multiple hours or days, acute bloody diarrhea, also known as dysentery, and finally, chronic or persistent diarrhea which lasts 2–4 weeks or more. There is normal growth with no evidence of malnutrition in the child experiencing persistent diarrhea. In chronic diarrhea there is no evidence of blood in the stool and there is no sign of infection. The condition may be related to irritable bowel syndrome. There are various tests that can be performed to rule out other causes of diarrhea that don't fall under the chronic criteria, including blood test, colonoscopy, and even genetic testing. Most acute or severe cases of diarrhea have treatment guidelines revolving around prescription or non prescription medications based on the cause, but the treatment protocols for chronic diarrhea focus on replenishing the body with lost fluids and electrolytes, because there typically isn't a treatable cause.
