Related Research Articles
Tetrahydrocannabinol (THC) is a cannabinoid found in cannabis. It is the principal psychoactive constituent of cannabis and one of at least 113 total cannabinoids identified on the plant. Its chemical formula C21H30O2 includes compounds, the term THC usually refers to the delta-9-THC isomer with chemical name (−)-trans-Δ9-tetrahydrocannabinol. It is a colorless oil.

The effects of cannabis are caused by chemical compounds in the cannabis plant, including 113 different cannabinoids such as tetrahydrocannabinol (THC) and 120 terpenes, which allow its drug to have various psychological and physiological effects on the human body. Different plants of the genus Cannabis contain different and often unpredictable concentrations of THC and other cannabinoids and hundreds of other molecules that have a pharmacological effect, so the final net effect cannot reliably be foreseen.

Medical cannabis, or medical marijuana (MMJ), is cannabis and cannabinoids that are prescribed by physicians for their patients. The use of cannabis as medicine has not been rigorously tested due to production and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.
Cannabinoids are several structural classes of compounds found in the cannabis plant primarily and most animal organisms or as synthetic compounds. The most notable cannabinoid is the phytocannabinoid tetrahydrocannabinol (THC) (delta-9-THC), the primary psychoactive compound in cannabis. Cannabidiol (CBD) is also a major constituent of temperate cannabis plants and a minor constituent in tropical varieties. At least 113 distinct phytocannabinoids have been isolated from cannabis, although only four have been demonstrated to have a biogenetic origin. It was reported in 2020 that phytocannabinoids can be found in other plants such as rhododendron, licorice and liverwort, and earlier in Echinacea.
Cannabinol (CBN) is a mildly psychoactive cannabinoid that acts as a low affinity partial agonist at both CB1 and CB2 receptors. This activity at CB1 and CB2 receptors constitutes interaction of CBN with the endocannabinoid system (ECS).

Cannabidiol (CBD) is a phytocannabinoid discovered in 1940. It is one of 113 identified cannabinoids in cannabis plants, along with tetrahydrocannabinol (THC), and accounts for up to 40% of the plant's extract. As of 2022, clinical research on CBD included studies related to the treatment of anxiety, addiction, psychosis, movement disorders, and pain, but there is insufficient high-quality evidence that cannabidiol is effective for these conditions. CBD is also sold as a herbal dietary supplement promoted with unproven claims of particular therapeutic effects.

Tetrahydrocannabivarin is a homologue of tetrahydrocannabinol (THC) having a propyl (3-carbon) side chain instead of pentyl (5-carbon), making it non-psychoactive in lower doses. It has been shown to exhibit neuroprotective activity, appetite suppression, glycemic control and reduced side effects compared to THC, making it a potential treatment for management of obesity and diabetes. THCV was studied by Roger Adams as early as 1942.
In the United States, the removal of cannabis from Schedule I of the Controlled Substances Act, the category reserved for drugs that have "no currently accepted medical use", is a proposed legal and administrative change in cannabis-related law at the federal level. After being proposed repeatedly since 1972, in 2024, the US Department of Justice announced it was initiating rulemaking to reschedule cannabis to Schedule III of the Controlled Substances Act.

Cannabis, also known as marijuana or weed among other names, is a psychoactive drug from the cannabis plant. Native to Central or South Asia, the cannabis plant has been used as a drug for both recreational and entheogenic purposes and in various traditional medicines for centuries. Tetrahydrocannabinol (THC) is the main psychoactive component of cannabis, which is one of the 483 known compounds in the plant, including at least 65 other cannabinoids, such as cannabidiol (CBD). Cannabis can be used by smoking, vaporizing, within food, or as an extract.

Nabilone, sold under the brand name Cesamet among others, is a synthetic cannabinoid with therapeutic use as an antiemetic and as an adjunct analgesic for neuropathic pain. It mimics tetrahydrocannabinol (THC), the primary psychoactive compound found naturally occurring in Cannabis.
Nabiximols is a specific Cannabis extract that was approved in 2010 as a botanical drug in the United Kingdom. Nabiximols is sold as a mouth spray intended to alleviate neuropathic pain, spasticity, overactive bladder, and other symptoms of multiple sclerosis; it was developed by the UK company GW Pharmaceuticals. In 2019, it was proposed that following application of the spray, nabiximols is washed away from the oral mucosa by the saliva flow and ingested into the stomach, with subsequent absorption from the gastro-intestinal tract. Nabiximols is a combination drug standardized in composition, formulation, and dose. Its principal active components are the cannabinoids: tetrahydrocannabinol (THC) and cannabidiol (CBD). Each spray delivers a dose of 2.7 mg THC and 2.5 mg CBD.

Cannabis tea is a cannabis-infused drink prepared by steeping various parts of the cannabis plant in hot or cold water. Cannabis tea is commonly recognized as an alternative form of preparation and consumption of the cannabis plant, more popularly known as marijuana, pot, or weed. This plant has long been recognized as an herbal medicine employed by health professionals worldwide to ease symptoms of disease, as well as a psychoactive drug used recreationally and in spiritual traditions. Though less commonly practiced than popular methods like smoking or consuming edibles, drinking cannabis tea can produce comparable physical and mental therapeutic effects. Such effects are largely attributed to the THC and CBD content of the tea, levels of which are drastically dependent on individual preparation techniques involving volume, amount of cannabis, and boiling time. Also in common with these administration forms of cannabis is the heating component performed before usage. Due to the rather uncommon nature of this particular practice of cannabis consumption in modern times as well as the legality of cannabis throughout the World, the research available on the composition of cannabis tea is limited and based broadly around what is known of cannabis as it exists botanically.

Geoffrey William Guy is a British pharmacologist, physician, businessman and academic, who co-founded GW Pharmaceuticals and has developed treatments using compounds found in cannabis, which are the first cannabis-based medicines approved by and available on the British National Health Service (NHS).
Cannabis strains are either pure or hybrid varieties of the plant genus Cannabis, which encompasses the species C. sativa, C. indica, and C. ruderalis.
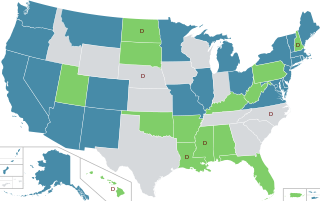
In the United States, the use of cannabis for medical purposes is legal in 38 states, four out of five permanently inhabited U.S. territories, and the District of Columbia, as of March 2023. Ten other states have more restrictive laws limiting THC content, for the purpose of allowing access to products that are rich in cannabidiol (CBD), a non-psychoactive component of cannabis. There is significant variation in medical cannabis laws from state to state, including how it is produced and distributed, how it can be consumed, and what medical conditions it can be used for.
Dronabinol (INN), also known under the trade names Marinol and Syndros, is a generic name for the molecule of delta-9-tetrahydrocannabinol in the pharmaceutical context. It has indications as an appetite stimulant, antiemetic, and sleep apnea reliever and is approved by the FDA as safe and effective for HIV/AIDS-induced anorexia and chemotherapy-induced nausea and vomiting only.
The long-term effects of cannabis have been the subject of ongoing debate. Because cannabis is illegal in most countries, clinical research presents a challenge and there is limited evidence from which to draw conclusions. In 2017, the U.S. National Academies of Sciences, Engineering, and Medicine issued a report summarizing much of the published literature on health effects of cannabis, into categories regarded as conclusive, substantial, moderate, limited and of no or insufficient evidence to support an association with a particular outcome.
Charlotte's Web is a brand of high-cannabidiol (CBD), low-tetrahydrocannabinol (THC) products derived from industrial hemp and marketed as dietary supplements and cosmetics under federal law of the United States. It is produced by Charlotte's Web, Inc. in Colorado. Hemp-derived products do not induce the psychoactive "high" typically associated with recreational marijuana strains that are high in THC. Charlotte's Web hemp-derived products contain less than 0.3% THC.
The Cannabinoid Research Initiative of Saskatchewan (CRIS) was founded in 2017 as an interdisciplinary research team of clinician researchers (medical and veterinary), basic scientists, and social scientists. CRIS aims to obtain scientific evidence about the application of Cannabinoids and Medical cannabis to humans and animals, for health, disease and disorders. The team was initially based at the University of Saskatchewan, in Saskatoon, Saskatchewan, Canada but includes researchers based at the University of Regina and University of Alberta. A strategic management executive committee coordinates activities and develops research opportunities. The sections of CRIS include: Analytical Evaluations, Human Clinical Studies, Biomedical studies, Veterinary Sciences, Knowledge Translation and Studies of Cannabinoids and Society. CRIS members participate in the Canadian Consortium for the Investigation of Cannabinoids, and the International Cannabinoid Research Society.

Δ-8-tetrahydrocannabinol is a psychoactive cannabinoid found in the Cannabis plant. It is an isomer of delta-9-tetrahydrocannabinol, the compound commonly known as THC, with which it co-occurs in hemp; natural quantities of ∆8-THC found in hemp are low.
References
- 1 2 3 4 Sagy, Iftach; Peleg-Sagy, Tal; Barski, Leonid; Zeller, Lior; Jotkowitz, Alan (March 2018). "Ethical issues in medical cannabis use". European Journal of Internal Medicine. 49: 20–22. doi:10.1016/j.ejim.2018.01.016. PMID 29482739.
- 1 2 Hudak, John; Wallack, Grace (October 2015), "Ending the U.S. government's war on medical marijuana research" (PDF), Center for Effective Public Management at Brookings, The Brookings Institution, archived (PDF) from the original on 2017-12-29, retrieved 2018-04-01
- 1 2 3 The Obstruction Of Medical Cannabis Research In The U.S. (PDF), Americans for Safe Access, April 2009, archived from the original (PDF) on 2017-10-19, retrieved 2018-04-01
- ↑ Zielinski, Alex (17 August 2016). "The DEA Hasn't Made Marijuana Research Any Easier". ThinkProgress. Archived from the original on 7 September 2017. Retrieved 1 July 2017.
- 1 2 3 The DEA: Four Decades of Impeding And Rejecting Science (PDF), Drug Policy Alliance / Multidisciplinary Associations for Psychedelic Studies, June 2014, archived (PDF) from the original on 2017-12-19, retrieved 2018-04-01
- 1 2 "Marijuana research: Overcoming the barriers". American Psychological Association. 14 September 2017. Archived from the original on 4 October 2017. Retrieved 9 October 2017.
- 1 2 Nelson, Steven (22 June 2015). "Major Pot Research Barrier Goes Up in Smoke". U.S. News & World Report. Archived from the original on 19 October 2017. Retrieved 29 June 2017.
- ↑ Ferro, Shaunacy (13 April 2013). "Why It's So Hard For Scientists To Study Medical Marijuana". Popular Science. Archived from the original on 24 April 2013. Retrieved 9 October 2017.
- ↑ Hellerman, Caleb (8 March 2017). "Scientists say the government's only pot farm has moldy samples — and no federal testing standards". PBS. Archived from the original on 8 October 2017. Retrieved 9 October 2017.
- ↑ Hudak, John (11 August 2016). "The DEA's marijuana decision is more important than rescheduling". The Brookings Institution. Archived from the original on 19 October 2017. Retrieved 9 October 2017.
- ↑ Gurman, Sadie (May 14, 2021). "Marijuana Medical Research Growers Receive U.S. Approval". The Wall Street Journal. Archived from the original on May 15, 2021. Retrieved August 24, 2022.
- ↑ "Marihuana Growers Information". usdoj.gov. Archived from the original on August 24, 2022. Retrieved August 24, 2022.
- ↑ Nelson, Steven (August 11, 2016). "DEA Ends Half-Century Pot Monopoly, But Withholds Big Prize for Reformers". U.S. News & World Report. Archived from the original on August 25, 2022. Retrieved August 24, 2022.
- ↑ "Marijuana -- AAFP Policies". aafp.org. Archived from the original on 10 December 2017. Retrieved 30 July 2017.
- ↑ American Academy of Pediatrics Reaffirms Opposition to Legalizing Marijuana for Recreational or Medical Use, American Academy of Pediatrics, 26 January 2015, archived from the original on 26 April 2018, retrieved 30 July 2017
- ↑ "Marijuana and Cancer". American Cancer Society. Archived from the original on 22 June 2017. Retrieved 12 July 2017.
- ↑ Fasinu PS, Phillips S, ElSohly MA, Walker LA (2016). "Current Status and Prospects for Cannabidiol Preparations as New Therapeutic Agents". Pharmacotherapy. 36 (7): 781–96. doi: 10.1002/phar.1780 . PMID 27285147. S2CID 4880700.
- ↑ "Sanjay Gupta tells Jeff Sessions how marijuana can save lives from opioids". 2018-04-24. Archived from the original on 2018-05-18. Retrieved 2018-05-18.
- ↑ "CNN's Sanjay Gupta tells Jeff Sessions medical marijuana could curb opioid epidemic | TribLIVE". Archived from the original on 2018-05-18. Retrieved 2018-05-18.
- ↑ "WEED 4: Pot Vs Pills". YouTube.com. Archived from the original on 2023-04-20. Retrieved 2018-05-18.
- ↑ "Cannabis (marihuana, marijuana) and the cannabinoids". Health Canada. February 2013. Archived from the original on 3 June 2017. Retrieved 2 December 2013.
- 1 2 "Cannabis and Cannabinoids (PDQ®)". National Cancer Institute at the National Institutes of Health. National Cancer Institute. 2 August 2013. Archived from the original on 7 April 2014. Retrieved 24 August 2013.
- ↑ Wilkie, Gianna; Sakr, Bachir; Rizack, Tina (17 March 2016). "Medical Marijuana Use in Oncology". JAMA Oncology. 2 (5): 670–675. doi: 10.1001/jamaoncol.2016.0155 . PMID 26986677.
- 1 2 3 Arney, Kat (25 July 2012). "Cannabis, cannabinoids and cancer – the evidence so far". Cancer Research UK. Archived from the original on 11 February 2014. Retrieved 8 December 2013.
- ↑ Gurney J, Shaw C, Stanley J, Signal V, Sarfati D (2015). "Cannabis exposure and risk of testicular cancer: a systematic review and meta-analysis". BMC Cancer (Systematic review). 15: 897. doi: 10.1186/s12885-015-1905-6 . PMC 4642772 . PMID 26560314.
- ↑ Madras, Bertha (11 December 2015). "Update of Cannabis and its medical use" (PDF). World Health Organization. Archived (PDF) from the original on 10 May 2017. Retrieved 18 December 2016.
- ↑ Peprah K, McCormack S (2019). "Medical Cannabis for the Treatment of Dementia: A Review of Clinical Effectiveness and Guidelines". Canadian Agency for Drugs and Technologies in Health. PMID 31525011.
- ↑ Sidney S (November 2016). "Marijuana Use and Type 2 Diabetes Mellitus: a Review". Curr. Diab. Rep. 16 (11): 117. doi:10.1007/s11892-016-0795-6. PMID 27747490. S2CID 28905440.
- ↑ Di Marzo V, Piscitelli F, Mechoulam R (2011). "Cannabinoids and endocannabinoids in metabolic disorders with focus on diabetes". Diabetes - Perspectives in Drug Therapy (Review). Handbook of Experimental Pharmacology. Vol. 203. pp. 75–104. doi:10.1007/978-3-642-17214-4_4. ISBN 978-3-642-17213-7. PMID 21484568.
- ↑ Fisher M, White S, Varbiro G, et al. (2010). "The role of cannabis and cannabinoids in diabetes". The British Journal of Diabetes & Vascular Disease. 10 (6): 267–273. doi:10.1177/1474651410385860. Archived from the original on 2019-09-03. Retrieved 2019-09-03.
- ↑ Friedman D, Devinsky O (2015). "Cannabinoids in the Treatment of Epilepsy". N. Engl. J. Med. (Review). 373 (11): 1048–58. doi:10.1056/NEJMra1407304. PMID 26352816.
- ↑ Reddy, DS; Golub, V (19 January 2016). "The Pharmacological Basis of Cannabis Therapy for Epilepsy". The Journal of Pharmacology and Experimental Therapeutics. 357 (1): 45–55. doi: 10.1124/jpet.115.230151 . PMID 26787773.
- ↑ Pertwee RG (2012). "Targeting the endocannabinoid system with cannabinoid receptor agonists: pharmacological strategies and therapeutic possibilities". Philosophical Transactions of the Royal Society B: Biological Sciences (Review). 367 (1607): 3353–63. doi:10.1098/rstb.2011.0381. PMC 3481523 . PMID 23108552.
- ↑ "DEA.gov / Headquarters News Releases, 12/23/15". Archived from the original on 2017-01-17. Retrieved 2017-04-27.
- ↑ Ward, Andrew (9 January 2014). "GW raises nearly $90m to develop childhood epilepsy treatment". Financial Times. Archived from the original on 11 January 2014. Retrieved 20 January 2014.
- ↑ Jampel, Henry (10 August 2009). "Position statement on marijuana and the treatment of glaucoma". American Glaucoma Society. Archived from the original on 9 July 2015. Retrieved 30 November 2013.
- ↑ Yazulla S (Sep 2008). "Endocannabinoids in the retina: from marijuana to neuroprotection". Progress in Retinal and Eye Research (Review). 27 (5): 501–26. doi:10.1016/j.preteyeres.2008.07.002. PMC 2584875 . PMID 18725316.
- ↑ [ needs update ]Kogan NM, Mechoulam R (2007). "Cannabinoids in health and disease". Dialogues Clin Neurosci. 9 (4): 413–30. doi:10.31887/DCNS.2007.9.4/nkogan. PMC 3202504 . PMID 18286801.
- ↑ [ needs update ]Singer HS (2005). "Tourette's syndrome: from behaviour to biology". Lancet Neurol (Review). 4 (3): 149–59. doi:10.1016/S1474-4422(05)01012-4. PMID 15721825. S2CID 20181150.
- ↑ [ needs update ]Robertson MM (2000). "Tourette syndrome, associated conditions and the complexities of treatment". Brain (Review). 123 (3): 425–62. doi: 10.1093/brain/123.3.425 . PMID 10686169.
- 1 2 3 4 5 6 7 Curtis A, Clarke CE, Rickards HE (2009). "Cannabinoids for Tourette's Syndrome". Cochrane Database Syst Rev (Review). 2009 (4): CD006565. doi:10.1002/14651858.CD006565.pub2. PMC 7387115 . PMID 19821373.
- ↑ Iuvone T, Esposito G, De Filippis D, et al. (2009). "Cannabidiol: A promising drug for neurodegenerative disorders?". CNS Neuroscience & Therapeutics (Review). 15 (1): 65–75. doi:10.1111/j.1755-5949.2008.00065.x. PMC 6494021 . PMID 19228180.
- ↑ [ needs update ]Carter GT, Rosen BS (2001). "Marijuana in the management of amyotrophic lateral sclerosis". The American Journal of Hospice & Palliative Care (Review). 18 (4): 264–70. doi:10.1177/104990910101800411. PMID 11467101. S2CID 16167096.
- ↑ [ needs update ]Ashton CH, Moore PB, Gallagher P, Young AH (2005). "Cannabinoids in bipolar affective disorder: A review and discussion of their therapeutic potential". Journal of Psychopharmacology (Review, meta-analysis). 19 (3): 293–300. doi:10.1177/0269881105051541. PMID 15888515. S2CID 1144939.
- ↑ Ethan B Russo (5 September 2013). Cannabis and Cannabinoids: Pharmacology, Toxicology, and Therapeutic Potential. Routledge. p. 191. ISBN 978-1-136-61493-4.
- ↑ [ needs update ]Di Carlo G, Izzo AA (2003). "Cannabinoids for gastrointestinal diseases: potential therapeutic applications". Expert Opinion on Investigational Drugs (Review). 12 (1): 39–49. doi:10.1517/13543784.12.1.39. PMID 12517253. S2CID 21225474.
- ↑ Koppel, Barbara S., MD; et al. (29 April 2014). "Systematic review: Efficacy and safety of medical marijuana in selected neurologic disorders". Neurology . 82 (17): 1556–1563. doi:10.1212/wnl.0000000000000363. PMC 4011465 . PMID 24778283.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Naftali T, Mechulam R, Lev LB, Konikoff FM (2014). "Cannabis for inflammatory bowel disease". Dig Dis (Review). 32 (4): 468–74. doi:10.1159/000358155. PMID 24969296. S2CID 25309621.
- 1 2 Mechoulam R, Peters M, Murillo-Rodriguez E, Hanus LO (August 2007). "Cannabidiol--recent advances". Chemistry & Biodiversity (Review). 4 (8): 1678–92. doi:10.1002/cbdv.200790147. PMID 17712814. S2CID 3689072.
- ↑ Campos AC, Moreira FA, Gomes FV, Del Bel EA, Guimarães FS (December 2012). "Multiple mechanisms involved in the large-spectrum therapeutic potential of cannabidiol in psychiatric disorders". Philos. Trans. R. Soc. Lond. B Biol. Sci. (Review). 367 (1607): 3364–78. doi:10.1098/rstb.2011.0389. PMC 3481531 . PMID 23108553.
- ↑ Lakhan SE, Rowland M (2009). "Whole plant cannabis extracts in the treatment of spasticity in multiple sclerosis: a systematic review". BMC Neurology (Review). 9: 59. doi: 10.1186/1471-2377-9-59 . PMC 2793241 . PMID 19961570.
- ↑ "Researchers Are Looking at Cannabis as a Potential Way to Prevent COVID-19". Forbes . Archived from the original on 2020-06-29. Retrieved 2020-06-29.