
The National Institutes of Health, commonly referred to as NIH, is the primary agency of the United States government responsible for biomedical and public health research. It was founded in the late 1880s and is now part of the United States Department of Health and Human Services. Many NIH facilities are located in Bethesda, Maryland, and other nearby suburbs of the Washington metropolitan area, with other primary facilities in the Research Triangle Park in North Carolina and smaller satellite facilities located around the United States. The NIH conducts its own scientific research through the NIH Intramural Research Program (IRP) and provides major biomedical research funding to non-NIH research facilities through its Extramural Research Program.
The American Psychiatric Association (APA) is the main professional organization of psychiatrists and trainee psychiatrists in the United States, and the largest psychiatric organization in the world. It has more than 38,000 members who are involved in psychiatric practice, research, and academia representing a diverse population of patients in more than 100 countries. The association publishes various journals and pamphlets, as well as the Diagnostic and Statistical Manual of Mental Disorders (DSM). The DSM codifies psychiatric conditions and is used mostly in the United States as a guide for diagnosing mental disorders.

A medication is a drug used to diagnose, cure, treat, or prevent disease. Drug therapy (pharmacotherapy) is an important part of the medical field and relies on the science of pharmacology for continual advancement and on pharmacy for appropriate management.

Clinical trials are prospective biomedical or behavioral research studies on human participants designed to answer specific questions about biomedical or behavioral interventions, including new treatments and known interventions that warrant further study and comparison. Clinical trials generate data on dosage, safety and efficacy. They are conducted only after they have received health authority/ethics committee approval in the country where approval of the therapy is sought. These authorities are responsible for vetting the risk/benefit ratio of the trial—their approval does not mean the therapy is 'safe' or effective, only that the trial may be conducted.
Prescription drug list prices in the United States continually are among the highest in the world. The high cost of prescription drugs became a major topic of discussion in the 21st century, leading up to the American health care reform debate of 2009, and received renewed attention in 2015. One major reason for high prescription drug prices in the United States relative to other countries is the inability of government-granted monopolies in the American health care sector to use their bargaining power to negotiate lower prices, and the American payer ends up subsidizing the world's R&D spending on drugs.
The National Center for Complementary and Integrative Health (NCCIH) is a United States government agency which explores complementary and alternative medicine (CAM). It was initially created in 1991 as the Office of Alternative Medicine (OAM), and renamed the National Center for Complementary and Alternative Medicine (NCCAM) before receiving its current name in 2014. NCCIH is one of the 27 institutes and centers that make up the National Institutes of Health (NIH) within the United States Department of Health and Human Services.
An orphan drug is a pharmaceutical agent that is developed to treat certain rare medical conditions. An orphan drug would not be profitable to produce without government assistance, due to the small population of patients affected by the conditions. The conditions that orphan drugs are used to treat are referred to as orphan diseases. The assignment of orphan status to a disease and to drugs developed to treat it is a matter of public policy that depends on the legislation of the country.

The pharmaceutical industry is an industry in medicine that discovers, develops, produces, and markets pharmaceutical drugs for use as medications to be administered to patients, with the aim to cure and prevent diseases, or alleviate symptoms. Pharmaceutical companies may deal in generic or brand medications and medical devices. They are subject to a variety of laws and regulations that govern the patenting, testing, safety, efficacy using drug testing and marketing of drugs. The global pharmaceuticals market produced treatments worth $1,228.45 billion in 2020 and showed a compound annual growth rate (CAGR) of 1.8%.

Chelation therapy is a medical procedure that involves the administration of chelating agents to remove heavy metals from the body. Chelation therapy has a long history of use in clinical toxicology and remains in use for some very specific medical treatments, although it is administered under very careful medical supervision due to various inherent risks, including the mobilization of mercury and other metals through the brain and other parts of the body by the use of weak chelating agents that unbind with metals before elimination, exacerbating existing damage. To avoid mobilization, some practitioners of chelation use strong chelators, such as selenium, taken at low doses over a long period of time.

The Wellcome Trust is a charitable foundation focused on health research based in London, in the United Kingdom. It was established in 1936 with legacies from the pharmaceutical magnate Henry Wellcome to fund research to improve human and animal health. The aim of the Trust is to "support science to solve the urgent health challenges facing everyone." It had a financial endowment of £29.1 billion in 2020, making it the fourth wealthiest charitable foundation in the world. In 2012, the Wellcome Trust was described by the Financial Times as the United Kingdom's largest provider of non-governmental funding for scientific research, and one of the largest providers in the world. According to their annual report, the Wellcome Trust spent GBP £1.1Bn on charitable activities across their 2019/2020 financial year. According to the OECD, the Wellcome Trust's financing for 2019 development increased by 22% to US$327 million.
Pharmaceutical marketing is a branch of marketing science and practice focused on the communication, differential positioning and commercialization of pharmaceutical products, like specialist drugs, biotech drugs and over-the-counter drugs. By extension, this definition is sometimes also used for marketing practices applied to nutraceuticals and medical devices.
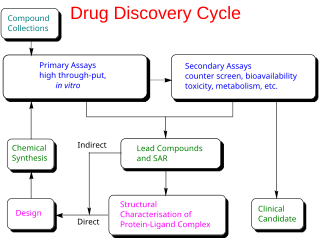
Drug development is the process of bringing a new pharmaceutical drug to the market once a lead compound has been identified through the process of drug discovery. It includes preclinical research on microorganisms and animals, filing for regulatory status, such as via the United States Food and Drug Administration for an investigational new drug to initiate clinical trials on humans, and may include the step of obtaining regulatory approval with a new drug application to market the drug. The entire process—from concept through preclinical testing in the laboratory to clinical trial development, including Phase I–III trials—to approved vaccine or drug typically takes more than a decade.
Medication costs, also known as drug costs are a common health care cost for many people and health care systems. Prescription costs are the costs to the end consumer. Medication costs are influenced by multiple factors such as patents, stakeholder influence, and marketing expenses. A number of countries including Canada, parts of Europe, and Brazil use external reference pricing as a means to compare drug prices and to determine a base price for a particular medication. Other countries use pharmacoeconomics, which looks at the cost/benefit of a product in terms of quality of life, alternative treatments, and cost reduction or avoidance in other parts of the health care system. Structures like the UK's National Institute for Health and Clinical Excellence and to a lesser extent Canada's Common Drug Review evaluate products in this way.
Medical ghostwriters are employed by pharmaceutical companies and medical-device manufacturers to produce apparently independent manuscripts for peer-reviewed journals, conference presentations and other communications. Physicians and other scientists are paid to attach their names to the manuscripts as though they had authored them. The named authors may have had little or no involvement in the research or writing process.
The Pediatric Trials Network (PTN) is a consortium of clinical research sites located around the United States that are cooperating in the design and conduct of clinical trials to improve medication labels affecting dosages for young patients. It conducts trials under the Best Pharmaceuticals for Children Act, passed in 2002. The network is sponsored by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
Clinical trials can be promoted and funded by a variety of sponsors, including pharmaceutical companies, government, research charities, foundations, medical organizations, and voluntary groups, such as patients' associations.
A physician-scientist is traditionally a holder of a medical degree and a doctor of philosophy also known as an MD-PhD. Compared to other clinicians, physician-scientists invest significant time and professional effort in scientific research and spend correspondingly less time in direct clinical practice with ratios of research to clinical time ranging from 50/50 to 80/20. Physician-scientists are often employed by academic or research institutions where they drive innovation across a wide range of medical specialties and may also use their extensive training to focus their clinical practices on specialized patient populations, such as those with rare genetic diseases or cancers. Although they are a minority of both practicing physicians and active research scientists, physician-scientists are often cited as playing a critical role in translational medicine and clinical research by adapting biomedical research findings to health care applications. Over time, the term physician scientist has expanded to holders of other clinical degrees—such as nurses, dentists, and veterinarians— who are also included by the United States National Institutes of Health in its studies of the physician-scientist workforce (PSW).

The 21st Century Cures Act is a United States law enacted by the 114th United States Congress in December 2016 and then signed into law on December 13, 2016. It authorized $6.3 billion in funding, mostly for the National Institutes of Health. The act was supported especially by large pharmaceutical manufacturers and was opposed especially by some consumer organizations.
The US carries out 46% of global research and development (R&D) in the life sciences, making it the world leader in medical research.
The cost of drug development is the full cost of bringing a new drug to market from drug discovery through clinical trials to approval. Typically, companies spend tens to hundreds of millions of U.S. dollars on drug development. One element of the complexity is that the much-publicized final numbers often not only include the out-of-pocket expenses for conducting a series of Phase I-III clinical trials, but also the capital costs of the long period during which the company must cover out-of-pocket costs for preclinical drug discovery. Additionally, companies often do not report whether a given figure includes the capitalized cost or comprises only out-of-pocket expenses, or both.



