Related Research Articles

Interstitial cystitis (IC), a type of bladder pain syndrome (BPS), is chronic pain in the bladder and pelvic floor of unknown cause. It is the urologic chronic pelvic pain syndrome of women. Symptoms include feeling the need to urinate right away, needing to urinate often, and pain with sex. IC/BPS is associated with depression and lower quality of life. Many of those affected also have irritable bowel syndrome and fibromyalgia.
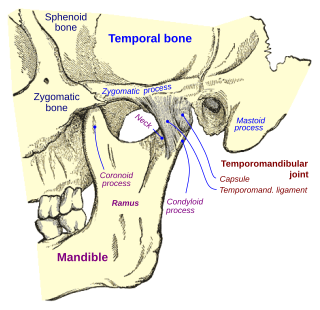
Temporomandibular joint dysfunction is an umbrella term covering pain and dysfunction of the muscles of mastication and the temporomandibular joints. The most important feature is pain, followed by restricted mandibular movement, and noises from the temporomandibular joints (TMJ) during jaw movement. Although TMD is not life-threatening, it can be detrimental to quality of life; this is because the symptoms can become chronic and difficult to manage.
Rheumatology is a branch of medicine devoted to the diagnosis and management of disorders whose common feature is inflammation in the bones, muscles, joints, and internal organs. Rheumatology covers more than 100 different complex diseases, collectively known as rheumatic diseases, which includes many forms of arthritis as well as lupus and Sjögren's syndrome. Doctors who have undergone formal training in rheumatology are called rheumatologists.

Fibromyalgia is a medical condition defined by the presence of chronic widespread pain, fatigue, waking unrefreshed, cognitive symptoms, lower abdominal pain or cramps, and depression. Other symptoms include insomnia and a general hypersensitivity.

Cyclobenzaprine, sold under the brand name Flexeril among others, is a muscle relaxer used for muscle spasms from musculoskeletal conditions of sudden onset. It is not useful in cerebral palsy. It is taken by mouth. Use is not recommended for more than a few weeks.

Piriformis syndrome is a condition which is believed to result from compression of the sciatic nerve by the piriformis muscle. The largest and most bulky nerve in the human body is the sciatic nerve. Starting at its origin it is 2 cm wide and 0.5 cm thick. The sciatic nerve forms the roots of L4-S3 segments of the lumbosacral plexus. The nerve will pass inferiorly to the piriformis muscle, in the direction of the lower limb where it divides into common tibial and fibular nerves. Symptoms may include pain and numbness in the buttocks and down the leg. Often symptoms are worsened with sitting or running.
Manual therapy, or manipulative therapy, is a physical treatment primarily used by physical therapists, physiotherapists, occupational therapists to treat musculoskeletal pain and disability; it mostly includes kneading and manipulation of muscles, joint mobilization and joint manipulation. It is also used by Rolfers, massage therapists, athletic trainers, osteopaths, and physicians.

Myofascial trigger points (MTrPs), also known as trigger points, are described as hyperirritable spots in the skeletal muscle. They are associated with palpable nodules in taut bands of muscle fibers. They are a topic of ongoing controversy, as there is limited data to inform a scientific understanding of the phenomenon. Accordingly, a formal acceptance of myofascial "knots" as an identifiable source of pain is more common among bodyworkers, physical therapists, chiropractors, and osteopathic practitioners. Nonetheless, the concept of trigger points provides a framework which may be used to help address certain musculoskeletal pain.

Costochondritis, also known as chest wall pain syndrome or costosternal syndrome, is a benign inflammation of the upper costochondral and sternocostal joints. 90% of patients are affected in multiple ribs on a single side, typically at the 2nd to 5th ribs. Chest pain, the primary symptom of costochondritis, is considered a symptom of a medical emergency, making costochondritis a common presentation in the emergency department. One study found costochondritis was responsible for 30% of patients with chest pain in an emergency department setting.
Medically unexplained physical symptoms are symptoms for which a treating physician or other healthcare providers have found no medical cause, or whose cause remains contested. In its strictest sense, the term simply means that the cause for the symptoms is unknown or disputed—there is no scientific consensus. Not all medically unexplained symptoms are influenced by identifiable psychological factors. However, in practice, most physicians and authors who use the term consider that the symptoms most likely arise from psychological causes. Typically, the possibility that MUPS are caused by prescription drugs or other drugs is ignored. It is estimated that between 15% and 30% of all primary care consultations are for medically unexplained symptoms. A large Canadian community survey revealed that the most common medically unexplained symptoms are musculoskeletal pain, ear, nose, and throat symptoms, abdominal pain and gastrointestinal symptoms, fatigue, and dizziness. The term MUPS can also be used to refer to syndromes whose etiology remains contested, including chronic fatigue syndrome, fibromyalgia, multiple chemical sensitivity and Gulf War illness.
Dry needling, also known as trigger point dry needling and intramuscular stimulation, is a treatment technique used by various healthcare practitioners, including physical therapists, physicians, and chiropractors, among others. Acupuncturists usually maintain that dry needling is adapted from acupuncture, but others consider dry needling as a variation of trigger point injections. It involves the use of either solid filiform needles or hollow-core hypodermic needles for therapy of muscle pain, including pain related to myofascial pain syndrome. Dry needling is mainly used to treat myofascial trigger points, but it is also used to target connective tissue, neural ailments, and muscular ailments. The American Physical Therapy Association defines dry needling as a technique used to treat dysfunction of skeletal muscle and connective tissue, minimize pain, and improve or regulate structural or functional damage.
Greater trochanteric pain syndrome (GTPS), a form of bursitis, is inflammation of the trochanteric bursa, a part of the hip.

Levator ani syndrome is a condition characterized by burning pain or tenesmus of the rectal or perineal area, caused by spasm of the levator ani muscle. The genesis of the syndrome is unknown; however, inflammation of the arcus tendon is a possible cause of levator ani syndrome.
Myotherapy is a form of muscle therapy which focuses on the assessment, treatment and rehabilitation of musculoskeletal pain and associated pathologies. The term myotherapy was originally coined by Bonnie Prudden to describe a specific type of trigger point therapy which she developed in the 1970s based on the earlier work of Travell and Simons who researched the cause and treatment of pain arising from myofascial trigger points. While based on rational principles, there is little scientific research regarding the efficacy of this therapy, so it remains controversial within the medical and academic disciplines.
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), previously known as chronic nonbacterial prostatitis, is long-term pelvic pain and lower urinary tract symptoms (LUTS) without evidence of a bacterial infection. It affects about 2–6% of men. Together with IC/BPS, it makes up urologic chronic pelvic pain syndrome (UCPPS).
In medicine, Carnett's sign is a finding on clinical examination in which (acute) abdominal pain remains unchanged or increases when the muscles of the abdominal wall are tensed. For this part of the abdominal examination, the patient can be asked to lift the head and shoulders from the examination table to tense the abdominal muscles. An alternative is to ask the patient to raise both legs with straight knees.
Dentomandibular sensorimotor dysfunction (DMSD) is a medical condition involving the mandible, upper three cervical (neck) vertebrae, and the surrounding muscle and nerve areas.
The term functional somatic syndrome (FSS) refers to a group of chronic diagnoses with no identifiable organic cause. This term was coined by Hemanth Samkumar. It encompasses disorders such as chronic fatigue syndrome, fibromyalgia, chronic widespread pain, temporomandibular disorder, irritable bowel syndrome, lower back pain, tension headache, atypical face pain, non-cardiac chest pain, insomnia, palpitation, dyspepsia and dizziness. General overlap exists between this term, somatization and somatoform.
Urologic chronic pelvic pain syndrome (UCPPS) is ongoing bladder pain in either sex, chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) in men and interstitial cystitis or painful bladder syndrome (IC/PBS) in women.
Fascial Manipulation is a manual therapy technique developed by Italian physiotherapist Luigi Stecco in the 1980s, aimed at evaluating and treating global fascial dysfunction by restoring normal motion/gliding to the system.
References
- 1 2 3 4 5 6 "Myofascial Pain Syndrome - Dental Disorders". Merck Manuals Professional Edition. Retrieved 27 May 2019.
- ↑ Bennett R (June 2007). "Myofascial pain syndromes and their evaluation". Best Practice & Research. Clinical Rheumatology. 21 (3): 427–445. doi:10.1016/j.berh.2007.02.014. PMID 17602992.
- ↑ "Myofascial Pain Syndrome". Made for this Moment. American Society of Anesthesiologists.
- ↑ Mayo Clinic Staff (3 Dec 2009). "Myofascial pain syndrome: Symptoms" . Retrieved 8 May 2011.
- 1 2 3 Bourgaize S, Newton G, Kumbhare D, Srbely J (April 2018). "A comparison of the clinical manifestation and pathophysiology of myofascial pain syndrome and fibromyalgia: implications for differential diagnosis and management" (PDF). The Journal of the Canadian Chiropractic Association. 62 (1): 26–41. PMC 6160895 . PMID 30270926.
- ↑ Tantanatip A, Chang KV (July 2022). "Myofascial Pain Syndrome.". StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. PMID 29763057.
- ↑ Quintner JL, Bove GM, Cohen ML (March 2015). "A critical evaluation of the trigger point phenomenon". Rheumatology. Rheumatology (Oxford). 2015 Mar;54(3):392-9. doi: 10.1093/rheumatology/keu471. Epub 2014 Dec 3. 54 (3): 392–399. doi: 10.1093/rheumatology/keu471 . PMID 25477053.
- ↑ Gerwin R (2005). "Differential Diagnosis of Trigger Points". Journal of Musculoskeletal Pain. 12 (3): 23–8. doi:10.1300/J094v12n03_04. S2CID 71224028.[ dead link ]
- ↑ Fricton JR, Kroening R, Haley D, Siegert R (December 1985). "Myofascial pain syndrome of the head and neck: a review of clinical characteristics of 164 patients". Oral Surgery, Oral Medicine, and Oral Pathology. 60 (6): 615–623. doi:10.1016/0030-4220(85)90364-0. PMID 3865133.
- ↑ de las Peñas CF, Campo MS, Carnero JF, Page JC (Jan 2005). "Manual therapies in myofascial trigger point treatment: a systematic review". Journal of Bodywork and Movement Therapies. 9 (1): 27–34. doi:10.1016/j.jbmt.2003.11.001.
- ↑ Starlanyl & Copeland 2001, p. 221.
- ↑ Harris RE, Clauw DJ (October 2002). "The use of complementary medical therapies in the management of myofascial pain disorders". Current Pain and Headache Reports. 6 (5): 370–374. doi:10.1007/s11916-002-0078-6. PMID 12357980. S2CID 41632904.
- ↑ Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM (January 2005). Furlan AD (ed.). "Acupuncture and dry-needling for low back pain". The Cochrane Database of Systematic Reviews (1): CD001351. doi:10.1002/14651858.CD001351.pub2. PMID 15674876.
- ↑ Starlanyl & Copeland 2001, p. 230.
- ↑ Borg-Stein J, Simons DG (March 2002). "Focused review: myofascial pain". Archives of Physical Medicine and Rehabilitation. 83 (3 Suppl 1): S40–S47. doi:10.1053/apmr.2002.32155. PMID 11973695.