Related Research Articles

In immunology, an antigen (Ag) is a molecule, moiety, foreign particulate matter, or an allergen, such as pollen, that can bind to a specific antibody or T-cell receptor. The presence of antigens in the body may trigger an immune response.
Immunotherapy or biological therapy is the treatment of disease by activating or suppressing the immune system. Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies, while immunotherapies that reduce or suppress are classified as suppression immunotherapies. Immunotherapy is under preliminary research for its potential to treat various forms of cancer.
An epitope, also known as antigenic determinant, is the part of an antigen that is recognized by the immune system, specifically by antibodies, B cells, or T cells. The part of an antibody that binds to the epitope is called a paratope. Although epitopes are usually non-self proteins, sequences derived from the host that can be recognized are also epitopes.
A cancer vaccine, or oncovaccine, is a vaccine that either treats existing cancer or prevents development of cancer. Vaccines that treat existing cancer are known as therapeutic cancer vaccines or tumor antigen vaccines. Some of the vaccines are "autologous", being prepared from samples taken from the patient, and are specific to that patient.
Cancer immunotherapy (immuno-oncotherapy) is the stimulation of the immune system to treat cancer, improving the immune system's natural ability to fight the disease. It is an application of the fundamental research of cancer immunology and a growing subspecialty of oncology.
Monoclonal antibodies (mAbs) have varied therapeutic uses. It is possible to create a mAb that binds specifically to almost any extracellular target, such as cell surface proteins and cytokines. They can be used to render their target ineffective, to induce a specific cell signal, to cause the immune system to attack specific cells, or to bring a drug to a specific cell type.
Ipilimumab, sold under the brand name Yervoy, is a monoclonal antibody medication that works to activate the immune system by targeting CTLA-4, a protein receptor that downregulates the immune system.
Antigenic escape, immune escape, immune evasion or escape mutation occurs when the immune system of a host, especially of a human being, is unable to respond to an infectious agent: the host's immune system is no longer able to recognize and eliminate a pathogen, such as a virus. This process can occur in a number of different ways of both a genetic and an environmental nature. Such mechanisms include homologous recombination, and manipulation and resistance of the host's immune responses.
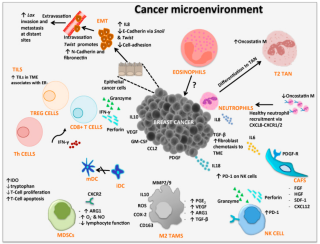
Cancer immunology (immuno-oncology) is an interdisciplinary branch of biology and a sub-discipline of immunology that is concerned with understanding the role of the immune system in the progression and development of cancer; the most well known application is cancer immunotherapy, which utilises the immune system as a treatment for cancer. Cancer immunosurveillance and immunoediting are based on protection against development of tumors in animal systems and (ii) identification of targets for immune recognition of human cancer.
Cancer/testis antigen 1 also known as LAGE2 or LAGE2B is a protein that in humans is encoded by the CTAG1B gene. It is most often referenced by its alias NY-ESO-1.
Peptide-based synthetic vaccines are subunit vaccines made from peptides. The peptides mimic the epitopes of the antigen that triggers direct or potent immune responses. Peptide vaccines can not only induce protection against infectious pathogens and non-infectious diseases but also be utilized as therapeutic cancer vaccines, where peptides from tumor-associated antigens are used to induce an effective anti-tumor T-cell response.
Gustav Gaudernack is a scientist working in the development of cancer vaccines and cancer immunotherapy. He has developed various strategies in immunological treatment of cancer. He is involved in several ongoing cellular and immuno-gene therapeutic clinical trials and his research group has put major efforts into the development of various T cell-based immunotherapeutic strategies.
Immunodominance is the immunological phenomenon in which immune responses are mounted against only a few of the antigenic peptides out of the many produced. That is, despite multiple allelic variations of MHC molecules and multiple peptides presented on antigen presenting cells, the immune response is skewed to only specific combinations of the two. Immunodominance is evident for both antibody-mediated immunity and cell-mediated immunity. Epitopes that are not targeted or targeted to a lower degree during an immune response are known as subdominant epitopes. The impact of immunodominance is immunodomination, where immunodominant epitopes will curtail immune responses against non-dominant epitopes. Antigen-presenting cells such as dendritic cells, can have up to six different types of MHC molecules for antigen presentation. There is a potential for generation of hundreds to thousands of different peptides from the proteins of pathogens. Yet, the effector cell population that is reactive against the pathogen is dominated by cells that recognize only a certain class of MHC bound to only certain pathogen-derived peptides presented by that MHC class. Antigens from a particular pathogen can be of variable immunogenicity, with the antigen that stimulates the strongest response being the immunodominant one. The different levels of immunogenicity amongst antigens forms what is known as dominance hierarchy.
Cancer/testis (CT) antigens are a group of proteins united by their importance in development and in cancer immunotherapy. In general, expression of these proteins is restricted to male germ cells in the adult animal. However, in cancer these developmental antigens are often re-expressed and can serve as a locus of immune activation. Thus, they are often classified as tumor antigens. The expression of CT antigens in various malignancies is heterogeneous and often correlates with tumor progression. CT antigens have been described in melanoma, liver cancer, lung cancer, bladder cancer, and pediatric tumors such as neuroblastoma. Gametogenesis offers an important role for many of these antigens in the differentiation, migration, and cell division of primordial germ cells, spermatogonia spermatocytes and spermatids. Because of their tumor-restricted expression and strong in vivo immunogenicity, CT antigens are identified as ideal targets for tumor specific immunotherapeutic approaches and prompted the development of several clinical trials of CT antigens-based vaccine therapy. CT antigens have been found to have at least 70 families so far, including about 140 members, most of which are expressed during spermatogenesis. Their expression are mainly regulated by epigenetic events, specifically, DNA methylation.
Individualized medicine tailors treatment to a single patient. The term refers to an individual, truly personalized medicine that strives to treat each patient on the basis of his own individual biology.
The mutanome is the entirety of somatic cancer mutations in an individual tumor.
Individualized cancer immunotherapy, also referred to as individualized immuno-oncology, is a novel concept for therapeutic cancer vaccines that are truly personalized to a single individual.

Uğur Şahin is a German oncologist and immunologist. He is the founder and CEO of BioNTech, which developed one of the major vaccines against COVID-19. His main fields of research are cancer research and immunology.

Özlem Türeci is a German physician, scientist and entrepreneur. In 2008, she co-founded the biotechnology company BioNTech, which in 2020 developed the first messenger RNA-based vaccine approved for use against COVID-19. Türeci has served as BioNTech's chief medical officer since 2018. Since 2021, she has been Professor of Personalized Immunotherapy at the Helmholtz Institute for Translational Oncology (HI-TRON) and Johannes Gutenberg University Mainz. Türeci and her spouse, Uğur Şahin, have won a number of awards.
Whole-cell vaccines are a type of vaccine that has been prepared in the laboratory from entire cells. Such vaccines simultaneously contain multiple antigens to activate the immune system. They induce antigen-specific T-cell responses.
References
- ↑ Leclerc M, Mezquita L, Guillebot De Nerville G, Tihy I, Malenica I, Chouaib S, Mami-Chouaib F (2019). "Recent Advances in Lung Cancer Immunotherapy: Input of T-Cell Epitopes Associated With Impaired Peptide Processing". Frontiers in Immunology. 10: 1505. doi: 10.3389/fimmu.2019.01505 . PMC 6616108 . PMID 31333652.
- ↑ Vormehr M, Diken M, Boegel S, Kreiter S, Türeci Ö, Sahin U (April 2016). "Mutanome directed cancer immunotherapy". Current Opinion in Immunology. 39: 14–22. doi:10.1016/j.coi.2015.12.001. PMID 26716729.
- ↑ Katsnelson A (February 2016). "Mutations as munitions: Neoantigen vaccines get a closer look as cancer treatment". Nature Medicine. 22 (2): 122–4. doi:10.1038/nm0216-122. PMID 26845402. S2CID 26454626.
- 1 2 Vormehr M, Türeci Ö, Sahin U (January 2019). "Harnessing Tumor Mutations for Truly Individualized Cancer Vaccines". Annual Review of Medicine. 70: 395–407. doi:10.1146/annurev-med-042617-101816. PMID 30691374. S2CID 59341051.
- ↑ Heemskerk B, Kvistborg P, Schumacher TN (January 2013). "The cancer antigenome". The EMBO Journal. 32 (2): 194–203. doi:10.1038/emboj.2012.333. PMC 3553384 . PMID 23258224.
- ↑ Gurjao C, Tsukrov D, Imakaev M, Luquette LJ, Mirny LA (2020-09-04). "Limited evidence of tumour mutational burden as a biomarker of response to immunotherapy". bioRxiv: 2020.09.03.260265. doi:10.1101/2020.09.03.260265. S2CID 221565320.
- ↑ Liu D, Schilling B, Liu D, Sucker A, Livingstone E, Jerby-Arnon L, et al. (December 2019). "Integrative molecular and clinical modeling of clinical outcomes to PD1 blockade in patients with metastatic melanoma". Nature Medicine. 25 (12): 1916–1927. doi:10.1038/s41591-019-0654-5. PMC 6898788 . PMID 31792460.
- ↑ Motzer RJ, Robbins PB, Powles T, Albiges L, Haanen JB, Larkin J, et al. (November 2020). "Avelumab plus axitinib versus sunitinib in advanced renal cell carcinoma: biomarker analysis of the phase 3 JAVELIN Renal 101 trial". Nature Medicine. 26 (11): 1733–1741. doi: 10.1038/s41591-020-1044-8 . PMC 8493486 . PMID 32895571.
- ↑ Wood MA, Weeder BR, David JK, Nellore A, Thompson RF (March 2020). "Burden of tumor mutations, neoepitopes, and other variants are weak predictors of cancer immunotherapy response and overall survival". Genome Medicine. 12 (1): 33. doi: 10.1186/s13073-020-00729-2 . PMC 7106909 . PMID 32228719.
- ↑ James EA, Pietropaolo M, Mamula MJ (June 2018). "Immune Recognition of β-Cells: Neoepitopes as Key Players in the Loss of Tolerance". Diabetes. 67 (6): 1035–1042. doi: 10.2337/dbi17-0030 . PMC 5961411 . PMID 29784651.
- ↑ Wilson EA, Anderson KS (December 2018). "Lost in the crowd: identifying targetable MHC class I neoepitopes for cancer immunotherapy". Expert Review of Proteomics. 15 (12): 1065–1077. doi:10.1080/14789450.2018.1545578. PMID 30408427. S2CID 53242832.
- ↑ Brennick CA, George MM, Corwin WL, Srivastava PK, Ebrahimi-Nik H (March 2017). "Neoepitopes as cancer immunotherapy targets: key challenges and opportunities". Immunotherapy. 9 (4): 361–371. doi: 10.2217/imt-2016-0146 . PMID 28303769.
- ↑ Feng YY, Griffith OL, Griffith M (August 2017). "Clinical implications of neoepitope landscapes for adult and pediatric cancers". Genome Medicine. 9 (1): 77. doi: 10.1186/s13073-017-0470-9 . PMC 5577778 . PMID 28854952.
- ↑ Saini SK, Rekers N, Hadrup SR (December 2017). "Novel tools to assist neoepitope targeting in personalized cancer immunotherapy". Annals of Oncology. 28 (suppl_12): xii3–xii10. doi: 10.1093/annonc/mdx544 . PMID 29092006.
- ↑ Türeci Ö, Vormehr M, Diken M, Kreiter S, Huber C, Sahin U (April 2016). "Targeting the Heterogeneity of Cancer with Individualized Neoepitope Vaccines". Clinical Cancer Research. 22 (8): 1885–96. doi: 10.1158/1078-0432.CCR-15-1509 . PMID 27084742.
- ↑ Sahin U, Derhovanessian E, Miller M, Kloke BP, Simon P, Löwer M, et al. (July 2017). "Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer". Nature. 547 (7662): 222–226. Bibcode:2017Natur.547..222S. doi: 10.1038/nature23003 . PMID 28678784.
- ↑ Ott PA, Hu Z, Keskin DB, Shukla SA, Sun J, Bozym DJ, et al. (July 2017). "An immunogenic personal neoantigen vaccine for patients with melanoma". Nature. 547 (7662): 217–221. Bibcode:2017Natur.547..217O. doi:10.1038/nature22991. PMC 5577644 . PMID 28678778.
- ↑ Hilf N, Kuttruff-Coqui S, Frenzel K, Bukur V, Stevanović S, Gouttefangeas C, et al. (January 2019). "Actively personalized vaccination trial for newly diagnosed glioblastoma". Nature. 565 (7738): 240–245. Bibcode:2019Natur.565..240H. doi:10.1038/s41586-018-0810-y. PMID 30568303. S2CID 56480674.
- ↑ Keskin DB, Anandappa AJ, Sun J, Tirosh I, Mathewson ND, Li S, et al. (January 2019). "Neoantigen vaccine generates intratumoral T cell responses in phase Ib glioblastoma trial". Nature. 565 (7738): 234–239. doi:10.1038/s41586-018-0792-9. PMC 6546179 . PMID 30568305.