This article's factual accuracy may be compromised due to out-of-date information. Please help update this article to reflect recent events or newly available information.(May 2013)
According to Michael First of the DSM-5 working committee[1] the focus of a relational disorder, in contrast to other DSM-IV disorders, "is on the relationship rather than on any one individual in the relationship".[2]
Relational disorders involve two or more individuals and a disordered "juncture", whereas typical Axis I psychopathology describes a disorder at the individual level. An additional criterion for a relational disorder is that the disorder cannot be due solely to a problem in one member of the relationship, but requires pathological interaction from each of the individuals involved in the relationship.[2]
For example, if a parent is withdrawn from one child but not another, the dysfunction could be attributed to a relational disorder. In contrast, if a parent is withdrawn from both children, the dysfunction may be more appropriately attributable to a disorder at the individual level.[3]
First states that "relational disorders share many elements in common with other disorders: there are distinctive features for classification; they can cause clinically significant impairment; there are recognizable clinical courses and patterns of comorbidity; they respond to specific treatments; and they can be prevented with early interventions. Specific tasks in a proposed research agenda: develop assessment modules; determine the clinical utility of relational disorders; determine the role of relational disorders in the etiology and maintenance of individual disorders; and consider aspects of relational disorders that might be modulated by individual disorders."[2]
The proposed new diagnosis defines a relational disorder as "persistent and painful patterns of feelings, behaviors, and perceptions" among two or more people in an important personal relationship, such a husband and wife, or a parent and children.[4]
The idea of a psychology of relational disorders is far from new. According to Adam Blatner, MD,[5] some of the early psychoanalysts alluded to it more or less directly, and the history of marital couple therapy began with a few pioneers in 1930s. J.L. Moreno, the inventor of psychodrama and a major pioneer of group psychotherapy and social psychology, noted the idea that relationships could be "sick" even if the people involved were otherwise "healthy," and even vice versa: Otherwise "sick" people could find themselves in a mutually supportive and "healthy" relationship.[5]
Moreno's ideas may have influenced some of the pioneers of family therapy, but also there were developments in general science, namely, cybernetic theory, developed in the mid-1940s, and noting the nature of circularity and feedback in complex systems. By the 1950s, the idea that relationships themselves could be problematic became quite apparent. So, diagnostically, in the sense not of naming a disease or disorder, but just helping people think through what was really going on, the idea of relational disorder was nothing new.[5]
Kinds
The majority of research on relational disorders concerns three relationship systems: adult children and their parents, minor children and their parents, and the marital relationship. There is also an increasing body of research on problems in dyadic gay relationships and on problematic sibling relationships.[6]
Marital
Marital disorders are divided into "Marital Conflict Disorder Without Violence" and "Marital Abuse Disorder (Marital Conflict Disorder With Violence)."[7] Couples with marital disorders sometimes come to clinical attention because the couple recognize long-standing dissatisfaction with their marriage and come to the clinician on their own initiative or are referred by a health care professional. Secondly, there is serious violence in the marriage which is "usually the husband battering the wife".[8] In these cases the emergency room or a legal authority often is the first to notify the clinician.
Most importantly, marital violence "is a major risk factor for serious injury and even death and women in violent marriages are at much greater risk of being seriously injured or killed" (National Advisory Council on Violence Against Women 2000).[9] The authors of this study add that "There is current considerable controversy over whether male-to-female marital violence is best regarded as a reflection of male psychopathology and control or whether there is an empirical base and clinical utility for conceptualizing these patterns as relational."[9]
Recommendations for clinicians making a diagnosis of "Marital Relational Disorder" should include the assessment of actual or "potential" male violence as regularly as they assess the potential for suicide in depressed patients. Further, "clinicians should not relax their vigilance after a battered wife leaves her husband, because some data suggest that the period immediately following a marital separation is the period of greatest risk for the women.
Many men will stalk and batter their wives in an effort to get them to return or punish them for leaving. Initial assessments of the potential for violence in a marriage can be supplemented by standardized interviews and questionnaires, which have been reliable and valid aids in exploring marital violence more systematically."[9]
The authors conclude with what they call "very recent information"[10] on the course of violent marriages which suggests that "over time a husband's battering may abate somewhat, but perhaps because he has successfully intimidated his wife."
The risk of violence remains strong in a marriage in which it has been a feature in the past. Thus, treatment is essential here; the clinician cannot just wait and watch.[10] The most urgent clinical priority is the protection of the wife because she is the one most frequently at risk, and clinicians must be aware that supporting assertiveness by a battered wife may lead to more beatings or even death.[10]
In some cases, men are abuse victims of their wives; there is not exclusively male-on-female physical violence, although this is more common than female-on-male violence.
Parent–child abuse
Research on parent–child abuse bears similarities to that on marital violence, with the defining characteristic of the disorder being physical aggression by a parent toward a child. The disorder is frequently concealed by parent and child, but may come to the attention of the clinician in several ways, from emergency room medical staff to reports from child protection services.[10]
Some features of abusive parent–child relationships that serve as a starting point for classification include: (a) the parent is physically aggressive with a child, often producing physical injury, (b) parent–child interaction is coercive, and parents are quick to react to provocations with aggressive responses, and children often reciprocate aggression, (c) parents do not respond effectively to positive or prosocial behavior in the child, (d) parents do not engage in discussion about emotions, (e) parent engages in deficient play behavior, ignores the child, rarely initiates play, and does little teaching, (f) children are insecurely attached and, where mothers have a history of physical abuse, show distinctive patterns of disorganized attachment, and (g) parents relationship shows coercive marital interaction patterns.[11]
Defining the relational aspects of these disorders can have important consequences. For example, in the case of early appearing feeding disorders, attention to relational problems may help delineate different types of clinical problems within an otherwise broad category. In the case of conduct disorder, the relational problems may be so central to the maintenance, if not the etiology, of the disorder that effective treatment may be impossible without recognizing and delineating it.[11]
↑ First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002). Personality Disorders and Relational Disorders, p. 161. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
↑ First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002). Personality Disorders and Relational Disorders, pp. 164, 166. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
↑ First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002). Personality Disorders and Relational Disorders, p. 163. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
1 2 3 First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002). Personality Disorders and Relational Disorders. p. 166. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
1 2 3 4 First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002) Personality Disorders and Relational Disorders. p. 167, 168. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
1 2 First, M.B., Bell, C.C., Cuthbert, B., Krystal, J.H., Malison, R., Offord, D.R., Riess, D., Shea, T., Widiger, T., Wisner, K.L. (2002). Personality Disorders and Relational Disorders, p. 169. Chapter 4 of Kupfer, D.J., First, M.B., & Regier, D.A.: A Research Agenda For DSM-V. Published by American Psychiatric Association
The Diagnostic and Statistical Manual of Mental Disorders is a publication by the American Psychiatric Association (APA) for the classification of mental disorders using a common language and standard criteria. It is the main book for the diagnosis and treatment of mental disorders in the United States and is considered one of the principal guides of psychiatry, along with the ICD, CCMD, and the Psychodynamic Diagnostic Manual. However, not all providers rely on the DSM-5 as a guide, since the ICD's mental disorder diagnoses are used around the world and scientific studies often measure changes in symptom scale scores rather than changes in DSM-5 criteria to determine the real-world effects of mental health interventions.
Borderline personality disorder (BPD), also known as emotionally unstable personality disorder (EUPD), is a personality disorder characterized by a long-term pattern of intense and unstable interpersonal relationships, distorted sense of self, and strong emotional reactions. Those affected often engage in self-harm and other dangerous behaviors, often due to their difficulty with returning their emotional level to a healthy or normal baseline. They may also struggle with a feeling of emptiness, fear of abandonment, and dissociation.
Histrionic personality disorder (HPD) is defined by the American Psychiatric Association as a personality disorder characterized by a pattern of excessive attention-seeking behaviors, usually beginning in early adulthood, including inappropriate seduction and an excessive desire for approval. People diagnosed with the disorder are said to be lively, dramatic, vivacious, enthusiastic, extroverted and flirtatious.
Antisocial personality disorder is a personality disorder characterized by a limited capacity for empathy and a long-term pattern of disregard or violation of the rights of others. Other notable symptoms include impulsivity and reckless behavior, a lack of remorse after hurting others, deceitfulness, irresponsibility, and aggressive behavior.
Hypoactive sexual desire disorder (HSDD), hyposexuality or inhibited sexual desire (ISD) is sometimes considered a sexual dysfunction, and is characterized as a lack or absence of sexual fantasies and desire for sexual activity, as judged by a clinician. For this to be regarded as a disorder, it must cause marked distress or interpersonal difficulties and not be better accounted for by another mental disorder, a drug, or some other medical condition. A person with ISD will not start, or respond to their partner's desire for, sexual activity. HSDD affects approximately 10% of all pre-menopausal women in the United States, or about 6 million women.
Reactive attachment disorder (RAD) is described in clinical literature as a severe and relatively uncommon disorder that can affect children, although these issues do occasionally persist into adulthood. RAD is characterized by markedly disturbed and developmentally inappropriate ways of relating socially in most contexts. It can take the form of a persistent failure to initiate or respond to most social interactions in a developmentally appropriate way—known as the "inhibited form". In the DSM-5, the "disinhibited form" is considered a separate diagnosis named "disinhibited attachment disorder".
Psychological trauma is an emotional response caused by severe distressing events such as accidents, violence, sexual assault, terror, or sensory overload.
Oppositional defiant disorder (ODD) is listed in the DSM-5 under Disruptive, impulse-control, and conduct disorders and defined as "a pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness". This behavior is usually targeted toward peers, parents, teachers, and other authority figures. Unlike conduct disorder (CD), those with ODD do not show patterns of aggression towards people or animals, destruction of property, theft, or deceit. One half of children with ODD also fulfill the diagnostic criteria for ADHD.
Complex post-traumatic stress disorder (CPTSD) is a stress-related mental disorder generally occurring in response to complex traumas, i.e. commonly prolonged or repetitive exposures to a series of traumatic events, within which individuals perceive little or no chance to escape.
Self-defeating personality disorder was a proposed personality disorder. As a descriptor for Other personality disorder it was mentioned in the DSM-III in 1980. It was discussed in an appendix of the revised third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) in 1987, but was never formally admitted into the manual. The distinction was not seen as clinically valuable because of its significant overlap with other personality disorders. It was entirely excluded from the DSM-IV. Since the DSM-5, the diagnoses other specified personality disorder and unspecified personality disorder have mostly replaced its use.
The Structured Clinical Interview for DSM (SCID) is a semi-structured interview guide for making diagnoses according to the diagnostic criteria published in the Diagnostic and Statistical Manual of Mental Disorders (DSM). The development of SCID has followed the evolution of the DSM and multiple versions are available for a single edition covering different categories of mental disorders. The first SCID was released in 1989, SCID-IV was published in 1994 and the current version, SCID-5, is available since 2013.
Child and adolescent psychiatry is a branch of psychiatry that focuses on the diagnosis, treatment, and prevention of mental disorders in children, adolescents, and their families. It investigates the biopsychosocial factors that influence the development and course of psychiatric disorders and treatment responses to various interventions. Child and adolescent psychiatrists primarily use psychotherapy and/or medication to treat mental disorders in the pediatric population.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is the 2013 update to the Diagnostic and Statistical Manual of Mental Disorders, the taxonomic and diagnostic tool published by the American Psychiatric Association (APA). In 2022, a revised version (DSM-5-TR) was published. In the United States, the DSM serves as the principal authority for psychiatric diagnoses. Treatment recommendations, as well as payment by health care providers, are often determined by DSM classifications, so the appearance of a new version has practical importance. However, not all providers rely on the DSM-5 for planning treatment as the ICD's mental disorder diagnoses are used around the world and scientific studies often measure changes in symptom scale scores rather than changes in DSM-5 criteria to determine the real-world effects of mental health interventions. The DSM-5 is the only DSM to use an Arabic numeral instead of a Roman numeral in its title, as well as the only living document version of a DSM.
Personality disorders (PD) are a class of mental disorders characterized by enduring maladaptive patterns of behavior, cognition, and inner experience, exhibited across many contexts and deviating from those accepted by the individual's culture. These patterns develop early, are inflexible, and are associated with significant distress or disability. The definitions vary by source and remain a matter of controversy. Official criteria for diagnosing personality disorders are listed in the sixth chapter of the International Classification of Diseases (ICD) and in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM).
Daniel S. Schechter is an American and Swiss psychiatrist known for his clinical work and research on intergenerational transmission or "communication" of violent trauma and related psychopathology involving parents and very young children. His published work in this area following the terrorist attacks on the World Trade Center in New York of September 11, 2001 led to a co-edited book entitled "September 11: Trauma and Human Bonds" (2003) and additional original articles with clinical psychologist Susan Coates that were translated into multiple languages and remain among the first accounts of 9/11 related loss and trauma described by mental health professionals who also experienced the attacks and their aftermath Schechter observed that separation anxiety among infants and young children who had either lost or feared loss of their caregivers triggered posttraumatic stress symptoms in the surviving caregivers. These observations validated his prior work on the adverse impact of family violence on the early parent-child relationship, formative social-emotional development and related attachment disturbances involving mutual dysregulation of emotion and arousal. This body of work on trauma and attachment has been cited by prominent authors in the attachment theory, psychological trauma, developmental psychobiology and neuroscience literatures
Michael B. First is an American psychiatrist who focuses on diagnostic criteria for mental disorders. He is Professor of Clinical Psychiatry at Columbia University. First was one of the editors of DSM-IV-TR, the Editor of Text and Criteria for the DSM-IV, and the editor of the Structured Clinical Interview for DSM-IV. He also served as consultant to the World Health Organization for the revision of ICD-11.
Allen J. Frances is an American psychiatrist. He is currently Professor and Chairman Emeritus of the Department of Psychiatry and Behavioral Sciences at Duke University School of Medicine. He is best known for serving as chair of the American Psychiatric Association task force overseeing the development and revision of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Frances is the founding editor of two well-known psychiatric journals: the Journal of Personality Disorders and the Journal of Psychiatric Practice.
In personality pathology, dimensional models of personality disorders conceptualize personality disorders as quantitatively rather than qualitatively different from normal personality. They consist of extreme, maladaptive levels of certain personality characteristics. Within the context of personality psychology, a "dimension" refers to a continuum on which an individual can have various levels of a characteristic, in contrast to the dichotomous categorical approach in which an individual does or does not possess a characteristic. According to dimensional models personality disorders are classified according to which characteristics are expressed at which levels. This stands in contrast to the traditional categorical models of classification, which are based on the boolean presence or absence of symptoms and do not take into account levels of expression of a characteristic or the presence of any underlying dimension.
Augustus John Rush is an internationally renowned psychiatrist. He is a professor emeritus in Duke-NUS Medical School at the National University of Singapore (NUS), and adjunct professor of psychiatry and behavioral sciences at Duke University School of Medicine. He has authored and edited more than 10 books, and over 600 scientific journal articles that are largely focused on the diagnosis and treatment of depressive and bipolar disorders.
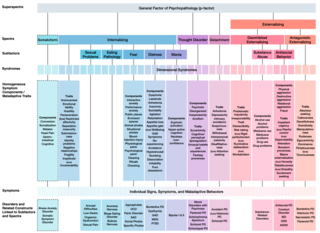
The Hierarchical Taxonomy Of Psychopathology (HiTOP) consortium was formed in 2015 as a grassroots effort to articulate a classification of mental health problems based on recent scientific findings on how the components of mental disorders fit together. The consortium is developing the HiTOP model, a classification system, or taxonomy, of mental disorders, or psychopathology, aiming to prioritize scientific results over convention and clinical opinion. The motives for proposing this classification were to aid clinical practice and mental health research. The consortium was organized by Drs. Roman Kotov, Robert Krueger, and David Watson. At inception it included 40 psychologists and psychiatrists, who had a record of scientific contributions to classification of psychopathology The HiTOP model aims to address limitations of traditional classification systems for mental illness, such as the DSM-5 and ICD-10, by organizing psychopathology according to evidence from research on observable patterns of mental health problems.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.