Related Research Articles

A copycat suicide is defined as an emulation of another suicide that the person attempting suicide knows about either from local knowledge or due to accounts or depictions of the original suicide on television and in other media. The publicized suicide serves as a trigger, in the absence of protective factors, for the next suicide by a susceptible or suggestible person. This is referred to as suicide contagion.

Self-harm is intentional behavior that is considered harmful to oneself. This is most commonly regarded as direct injury of one's own skin tissues usually without a suicidal intention. Other terms such as cutting, self-injury, and self-mutilation have been used for any self-harming behavior regardless of suicidal intent. Common forms of self-harm include damaging the skin with a sharp object or by scratching, hitting, or burning. The exact bounds of self-harm are imprecise, but generally exclude tissue damage that occurs as an unintended side-effect of eating disorders or substance abuse, as well as societally acceptable body modification such as tattoos and piercings.
Suicide prevention is a collection of efforts to reduce the risk of suicide. Suicide is often preventable, and the efforts to prevent it may occur at the individual, relationship, community, and society level. Suicide is a serious public health problem that can have long-lasting effects on individuals, families, and communities. Preventing suicide requires strategies at all levels of society. This includes prevention and protective strategies for individuals, families, and communities. Suicide can be prevented by learning the warning signs, promoting prevention and resilience, and committing to social change.
There are more than 700,000 estimated suicide deaths every year. Suicide affects every demographic, yet there are some populations that are more impacted than others. For example, among 15–29 year olds, suicide is much more prominent; this being the fourth leading cause of death within this age group.

Suicidal ideation, or suicidal thoughts, is the thought process of having ideas, or ruminations about the possibility of committing suicide. It is not a diagnosis but is a symptom of some mental disorders, use of certain psychoactive drugs, and can also occur in response to adverse life events without the presence of a mental disorder.
Suicide risk assessment is a process of estimating the likelihood for a person to attempt or die by suicide. The goal of a thorough risk assessment is to learn about the circumstances of an individual person with regard to suicide, including warning signs, risk factors, and protective factors. Risk for suicide is re-evaluated throughout the course of care to assess the patient's response to personal situational changes and clinical interventions. Accurate and defensible risk assessment requires a clinician to integrate a clinical judgment with the latest evidence-based practice, although accurate prediction of low base rate events, such as suicide, is inherently difficult and prone to false positives.
Youth suicide is when a young person, generally categorized as someone below the legal age of majority, deliberately ends their own life. Rates of youth suicide and attempted youth suicide in Western societies and other countries are high. Youth suicide attempts are more common among girls, but adolescent males are the ones who usually carry out suicide. Suicide rates in youths have nearly tripled between the 1960s and 1980s. For example, in Australia suicide is second only to motor vehicle accidents as its leading cause of death for people aged 15 to 25.

Suicide is the act of intentionally causing one's own death. Mental disorders, physical disorders, and substance abuse are risk factors. Some suicides are impulsive acts due to stress, relationship problems, or harassment and bullying. Those who have previously attempted suicide are at a higher risk for future attempts. Effective suicide prevention efforts include limiting access to methods of suicide such as firearms, drugs, and poisons; treating mental disorders and substance abuse; careful media reporting about suicide; improving economic conditions; and dialectical behaviour therapy (DBT). Although crisis hotlines are common resources, their effectiveness has not been well studied.
The American Association of Suicidology (AAS) is a 501(c)(3) nonprofit organization which advocates for suicide prevention. It was established in 1968 by Edwin S. Shneidman, who has been called "a pioneer in suicide prevention." Its official journal is Suicide and Life-Threatening Behavior, published six times a year by Wiley-Blackwell.
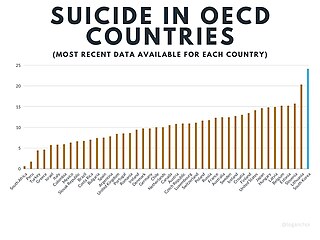
Suicide in South Korea occurs at the 12th highest rate in the world. South Korea has the highest recorded suicide rate in the OECD. In South Korea, it is estimated to affect 0.02 percent of the population by the WHO. In 2012, suicide was the fourth-highest cause of death. The suicide rate has consistently declined between 2012 and 2019, the year when the latest data are available.

Gender differences in suicide rates have been shown to be significant. There are different rates of suicides and suicidal behavior between males and females. While females more often have suicidal thoughts, males die by suicide more frequently. This discrepancy is also known as the gender paradox in suicide.
A suicide attempt is an act in which an individual tries to kill themselves but survives. Mental health professionals discourage describing suicide attempts as "failed" or "unsuccessful", as doing so may imply that a suicide resulting in death is a successful or desirable outcome.
Advocacy of suicide, also known as pro-suicide, has occurred in many cultures and subcultures.
Researchers study Social media and suicide to find if a correlation exists between the two. Some research has shown that there may be a correlation.
Bullying suicide are considered together when the cause of suicide is attributable to the victim having been bullied, either in person or via social media. Writers Neil Marr and Tim Field wrote about it in their 2001 book Bullycide: Death at Playtime.
The Columbia Suicide Severity Rating Scale, or C-SSRS, is a suicidal ideation and behavior rating scale created by researchers at Columbia University, University of Pennsylvania, University of Pittsburgh and New York University to evaluate suicide risk. It rates an individual's degree of suicidal ideation on a scale, ranging from "wish to be dead" to "active suicidal ideation with specific plan and intent and behaviors." Questions are phrased for use in an interview format, but the C-SSRS may be completed as a self-report measure if necessary. The scale identifies specific behaviors which may be indicative of an individual's intent to kill oneself. An individual exhibiting even a single behavior identified by the scale was 8 to 10 times more likely to die by suicide.
The relationship between antidepressant use and suicide risk is a subject of medical research and has faced varying levels of debate. This problem was thought to be serious enough to warrant intervention by the U.S. Food and Drug Administration to label greater likelihood of suicide as a risk of using antidepressants. Some studies have shown that the use of certain antidepressants correlate with an increased risk of suicide in some patients relative to other antidepressants. However, these conclusions have faced considerable scrutiny and disagreement: A multinational European study indicated that antidepressants decrease risk of suicide at the population level, and other reviews of antidepressant use claim that there is not enough data to indicate antidepressant use increases risk of suicide.
The interpersonal theory of suicide attempts to explain why individuals engage in suicidal behavior and to identify individuals who are at risk. It was developed by Thomas Joiner and is outlined in Why People Die By Suicide. The theory consists of three components that together lead to suicide attempts. According to the theory, the simultaneous presence of thwarted belongingness and perceived burdensomeness produce the desire for suicide. While the desire for suicide is necessary, it alone will not result in death by suicide. Rather, Joiner asserts that one must also have acquired capability to overcome one's natural fear of death.
Suicide awareness is a proactive effort to raise awareness around suicidal behaviors. It is focused on reducing social stigmas and ambiguity by bringing attention to suicide statistically and sociologically, and by encouraging positive dialogue and engagement to prevent suicide. Suicide awareness is linked to suicide prevention as both address suicide education and the dissemination of information to ultimately decrease the rate of suicide. Awareness is the first stage that can ease the need for prevention. Awareness signifies a fundamental consciousness of the threat, while prevention focuses on stopping the act. Suicide awareness is not a medical engagement but a combination of medical, social, emotional and financial counseling. Suicide awareness in adolescents focuses on the age group between 10–24 years, beginning with the onset of puberty.
Youth suicide in India is when young Indian people deliberately end their own life. People aged 15 to 24 years have the highest suicide rate in India, which is consistent with international trends in youth suicide. 35% of recorded suicides in India occur in this age group. Risk factors and methods of youth suicide differ from those in other age groups.
References
- ↑ Harris, Keith; McLean, John; Sheffield, Jeanie (July 2009), "Examining Suicide-Risk Individuals Who Go Online for Suicide-Related Purposes", Archives of Suicide Research, 13 (3): 264–276, doi:10.1080/13811110903044419, PMID 19591000, S2CID 205804938
- ↑ Mishara, Brian L.; Weisstub, David N. (2007), "Ethical, legal, and practical issues in the control and regulation of suicide promotion and assistance over the internet", Suicide and Life-Threatening Behavior, Suicide & life-threatening behavior, 37 (1): 58–65, doi:10.1521/suli.2007.37.1.58, ISSN 0363-0234, PMID 17397280
- ↑ Nick Britten and Richard Savill (23 Jan 2008), Police fear internet cult inspires teen suicides, Telegraph
- ↑ Prior, Trevor (August 2004), "Suicide Methods From the Internet", The American Journal of Psychiatry, Am J Psychiatry, 161 (8): 1500–1, doi:10.1176/appi.ajp.161.8.1500-a, PMID 15285986
- ↑ Kemp, C. G., & Collings, S. C. (2011). Hyperlinked suicide: Assessing the prominence and accessibility of suicide websites. Crisis, 32(3), 143-151. doi: 10.1027/0227-5910/a000068
- ↑ Harris, K. M. (2015). Life vs. death: The suicidal mind online. In E. Aboujaoude & V. Starcevic (Eds.), Mental Health in the Digital Age: Grave Dangers, Great Promise (pp. 135-151). New York, NY: Oxford University Press.