
In immunology, autoimmunity is the system of immune responses of an organism against its own healthy cells, tissues and other normal body constituents. Any disease resulting from this type of immune response is termed an "autoimmune disease". Prominent examples include celiac disease, diabetes mellitus type 1, Henoch–Schönlein purpura (HSP), systemic lupus erythematosus (SLE), Sjögren syndrome, eosinophilic granulomatosis with polyangiitis, Hashimoto's thyroiditis, Graves' disease, idiopathic thrombocytopenic purpura, Addison's disease, rheumatoid arthritis (RA), ankylosing spondylitis, polymyositis (PM), dermatomyositis (DM), and multiple sclerosis (MS). Autoimmune diseases are very often treated with steroids.
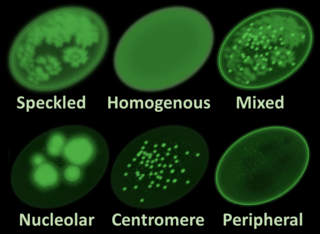
Antinuclear antibodies are autoantibodies that bind to contents of the cell nucleus. In normal individuals, the immune system produces antibodies to foreign proteins (antigens) but not to human proteins (autoantigens). In some cases, antibodies to human antigens are produced.
An autoantibody is an antibody produced by the immune system that is directed against one or more of the individual's own proteins. Many autoimmune diseases are associated with such antibodies.

Anti-mitochondrial antibodies (AMA) are autoantibodies, consisting of immunoglobulins formed against mitochondria, primarily the mitochondria in cells of the liver.
Extractable nuclear antigens (ENAs) are over 100 different soluble cytoplasmic and nuclear antigens. They are known as "extractable" because they can be removed from cell nuclei using saline and represent six main proteins: Ro, La, Sm, RNP, Scl-70, Jo1. Most ENAs are part of spliceosomes or nucleosomes complexes and are a type of small nuclear ribonucleoprotein (snRNPS). The location in the nucleus and association with spliceosomes or nucleosomes results in these ENAs being associated with additional RNA and proteins such as polymerases. This quality of ENAs often makes it difficult to purify and quantify their presence for clinical use.
Mixed connective tissue disease, commonly abbreviated as MCTD, is an autoimmune disease characterized by the presence of elevated blood levels of a specific autoantibody, now called anti-U1 ribonucleoprotein (RNP) together with a mix of symptoms of systemic lupus erythematosus (SLE), scleroderma, and polymyositis. The idea behind the "mixed" disease is that this specific autoantibody is also present in other autoimmune diseases such as systemic lupus erythematosus, polymyositis, scleroderma, etc. MCTD was characterized as an individual disease in 1972 by Sharp et al., and the term was introduced by Leroy in 1980.

Integrin alpha M (ITGAM) is one protein subunit that forms heterodimeric integrin alpha-M beta-2 (αMβ2) molecule, also known as macrophage-1 antigen (Mac-1) or complement receptor 3 (CR3). ITGAM is also known as CR3A, and cluster of differentiation molecule 11B (CD11B). The second chain of αMβ2 is the common integrin β2 subunit known as CD18, and integrin αMβ2 thus belongs to the β2 subfamily integrins.

Anti-cardiolipin antibodies (ACA) are antibodies often directed against cardiolipin and found in several diseases, including syphilis, antiphospholipid syndrome, livedoid vasculitis, vertebrobasilar insufficiency, Behçet's syndrome, idiopathic spontaneous abortion, and systemic lupus erythematosus (SLE). They are a form of anti-mitochondrial antibody. In SLE, anti-DNA antibodies and anti-cardiolipin antibodies may be present individually or together; the two types of antibodies act independently. This is in contrast to rheumatoid arthritis with systemic sclerosis (scleroderma) because anti-cardiolipin antibodies are present in both conditions, and therefore may tie the two conditions together.
Anti-topoisomerase antibodies (ATA) are autoantibodies directed against topoisomerase and found in several diseases, most importantly scleroderma. Diseases with ATA are autoimmune disease because they react with self-proteins. They are also referred to as anti-DNA topoisomerase I antibody.

Anti-thrombin antibodies are autoantibodies directed against thrombin that may constitute a fraction of lupus anticoagulant and are seen an increased levels in systemic lupus erythematosus.

Interferon alpha-1 is a protein that in humans is encoded by the IFNA1 gene.

Tripartite motif-containing protein 21, also known as E3 ubiquitin-protein ligase TRIM21, is a protein that in humans is encoded by the TRIM21 gene. Alternatively spliced transcript variants for this gene have been described but the full-length nature of only one has been determined. It is expressed in most human tissues.

60 kDa SS-A/Ro ribonucleoprotein is a protein that in humans is encoded by the TROVE2 gene.

Ficolin-3 is a protein that in humans is encoded by the FCN3 gene. Ficolin-3 was initially identified as H-ficolin, in which H is after the Hakata antigen that was previously found as an autoantigen in patients who lived in the city of Hakata.

Lupus erythematosus is a collection of autoimmune diseases in which the human immune system becomes hyperactive and attacks healthy tissues. Symptoms of these diseases can affect many different body systems, including joints, skin, kidneys, blood cells, heart, and lungs. The most common and most severe form is systemic lupus erythematosus.
RA33, also known as heterogeneous nuclear ribonucleoprotein A2/B1, is an autoantigen in human systemic autoimmune diseases.

Lupus, technically known as systemic lupus erythematosus (SLE), is an autoimmune disease in which the body's immune system mistakenly attacks healthy tissue in many parts of the body. Symptoms vary among people and may be mild to severe. Common symptoms include painful and swollen joints, fever, chest pain, hair loss, mouth ulcers, swollen lymph nodes, feeling tired, and a red rash which is most commonly on the face. Often there are periods of illness, called flares, and periods of remission during which there are few symptoms.
Anti-histone antibodies are autoantibodies that are a subset of the anti-nuclear antibody family, which specifically target histone protein subunits or histone complexes. They were first reported by Henry Kunkel, H.R. Holman, and H.R.G. Dreicher in their studies of cellular causes of lupus erythematosus in 1959–60. Today, anti-histone antibodies are still used as a marker for systemic lupus erythematosus, but are also implicated in other autoimmune diseases like Sjögren syndrome, dermatomyositis, or rheumatoid arthritis. Anti-histone antibodies can be used as a marker for drug-induced lupus.

Anti-SSA autoantibodies are a type of anti-nuclear autoantibodies that are associated with many autoimmune diseases, such as systemic lupus erythematosus (SLE), SS/SLE overlap syndrome, subacute cutaneous lupus erythematosus (SCLE), neonatal lupus and primary biliary cirrhosis. They are often present in Sjögren's syndrome (SS). Additionally, Anti-Ro/SSA can be found in other autoimmune diseases such as systemic sclerosis (SSc), polymyositis/dermatomyositis (PM/DM), rheumatoid arthritis (RA), and mixed connective tissue disease (MCTD), and are also associated with heart arrhythmia.
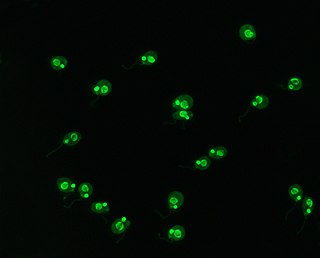
Crithidia luciliae is a flagellate parasite that uses the housefly, Musca domestica, as a host. As part of the family of Trypanosomatidae, it is characterised by the presence of a kinetoplast, a complex network of interlocking circular double-stranded DNA (dsDNA) molecules. The presence of the kinetoplast makes this organism important in the diagnosis of systemic lupus erythamatosus (SLE). By using C. luciliae as a substrate for immunofluorescence, the organelle can be used to detect anti-dsDNA antibodies, a common feature of the disease.
