Panniculitis is a group of diseases whose hallmark is inflammation of subcutaneous adipose tissue. Symptoms include tender skin nodules, and systemic signs such as weight loss and fatigue.

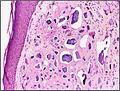
Dystrophic calcification (DC) is the calcification occurring in degenerated or necrotic tissue, as in hyalinized scars, degenerated foci in leiomyomas, and caseous nodules. This occurs as a reaction to tissue damage, including as a consequence of medical device implantation. Dystrophic calcification can occur even if the amount of calcium in the blood is not elevated, in contrast to metastatic calcification, which is a consequence of a systemic mineral imbalance, including hypercalcemia and/or hyperphosphatemia, that leads to calcium deposition in healthy tissues. In dystrophic calcification, basophilic calcium salt deposits aggregate, first in the mitochondria, then progressively throughout the cell. These calcifications are an indication of previous microscopic cell injury, occurring in areas of cell necrosis when activated phosphatases bind calcium ions to phospholipids in the membrane.

Calcinosis is the formation of calcium deposits in any soft tissue. It is a rare condition that has many different causes. These range from infection and injury to systemic diseases like kidney failure.
Sclerodactyly is a localized thickening and tightness of the skin of the fingers or toes that yields a characteristic claw-like appearance and spindle shape of the affected digits, and renders them immobile or of limited mobility. The thickened, discolored patches of skin are called morphea, and may involve connective tissue below the skin, as well as muscle and other tissues. Sclerodactyly is often preceded by months or even years by Raynaud's phenomenon when it is part of systemic scleroderma.

Angiokeratoma is a benign cutaneous lesion of capillaries, resulting in small marks of red to blue color and characterized by hyperkeratosis. Angiokeratoma corporis diffusum refers to Fabry's disease, but this is usually considered a distinct condition.

Granuloma annulare (GA) is a common, sometimes chronic skin condition which presents as reddish bumps on the skin arranged in a circle or ring. It can initially occur at any age, though two-thirds of patients are under 30 years old, and it is seen most often in children and young adults. Females are two times as likely to have it as males.
Leukemia cutis is the infiltration of neoplastic leukocytes or their precursors into the skin resulting in clinically identifiable cutaneous lesions. This condition may be contrasted with leukemids, which are skin lesions that occur with leukemia, but which are not related to leukemic cell infiltration. Leukemia cutis can occur in most forms of leukemia, including chronic myeloid leukemia, acute lymphoblastic leukemia, chronic lymphocytic leukemia, acute myeloid leukemia, and prolymphocytic leukemia.
Palisaded neutrophilic and granulomatous dermaititis (PNGS) is usually associated with a well-defined connective tissue disease, lupus erythematosus or rheumatoid arthritis most commonly, and often presents with eroded or ulcerated symmetrically distributed umbilicated papules or nodules on the elbows.

Infantile systemic hyalinosis is an allelic autosomal-recessive condition characterized by multiple skin nodules, hyaline deposition, gingival hypertrophy, osteolytic bone lesions and joint contractures.
Angiolipoleiomyoma is an acquired, solitary, asymptomatic acral nodule, characterized histologically by well-circumscribed subcutaneous tumors composed of smooth muscle cells, blood vessels, connective tissue, and fat.
Mucinoses are a group of cutaneous diseases caused by fibroblasts producing abnormally large amounts of acid mucopolysaccharides, usually hyaluronic acid.

Elephantiasis nostras is a disease that usually affects the lower legs or scrotum. Swelling is accompanied by rough nodules or wart-like plaques on the skin. If the disease is not treated, it eventually results in pain and immobility.

Cutaneous lymphoid hyperplasia refers to a groups of benign cutaneous disorders characterized by collections of lymphocytes, macrophages, and dendritic cells in the skin. Conditions included in this groups are:
Primary cutaneous marginal zone lymphomas represent a heterogeneous group of diseases characterized by solitary or multiple dermal or subcutaneous nodules. Lymphomas included in this group are:
Plasmacytosis is a condition in which there is an unusually large proportion of plasma cells in tissues, exudates, or blood. Plasmacytosis may be divided into two types—cutaneous and systemic—both of which have identical skin findings. Patients with plasmacytosis have been predominantly found to have lung infections whereas multiple myeloma is rarely found.
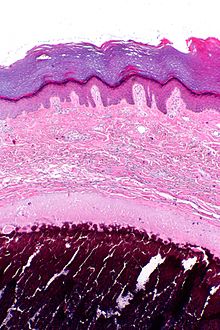
Idiopathic scrotal calcinosis is a cutaneous condition characterized by calcification of the skin resulting from the deposition of calcium and phosphorus occurring on the scrotum. However, the levels of calcium and phosphate in the blood are normal. Idiopathic scrotal calcinosis typically affects young males, with an onset between adolescence and early adulthood. The scrotal calcinosis appears, without any symptoms, as yellowish nodules that range in size from 1 mm to several centimeters.

Osteoma cutis is a cutaneous condition characterized by the presence of bone within the skin in the absence of a preexisting or associated lesion. Osteoma cutis often manifests as solid, varying-sized, skin-colored subcutaneous nodules.

A sebaceous adenoma, a type of adenoma, a cutaneous condition characterized by a slow-growing tumor usually presenting as a pink, flesh-coloured, or yellow papule or nodule.
Plate-like osteoma cutis is a congenital condition characterized by firm papules and nodules on the skin.