Related Research Articles

Asperger syndrome (AS), also known as Asperger's, was the name of a neurodevelopmental disorder no longer recognised as a diagnosis in itself, having been merged into autism spectrum disorder (ASD). It was characterized by significant difficulties in social interaction and nonverbal communication, along with restricted and repetitive patterns of behaviour and interests. It was said to differ from other diagnoses that were merged into ASD by relatively unimpaired language and intelligence. The syndrome was named after the Austrian pediatrician Hans Asperger, who, in 1944, described children in his care who struggled to form friendships, did not understand others' gestures or feelings, engaged in one-sided conversations about their favourite interests, and were clumsy.
Developmental disorders comprise a group of psychiatric conditions originating in childhood that involve serious impairment in different areas. There are several ways of using this term. The most narrow concept is used in the category "Specific Disorders of Psychological Development" in the ICD-10. These disorders comprise developmental language disorder, learning disorders, motor disorders, and autism spectrum disorders. In broader definitions ADHD is included, and the term used is neurodevelopmental disorders. Yet others include antisocial behavior and schizophrenia that begins in childhood and continues through life. However, these two latter conditions are not as stable as the other developmental disorders, and there is not the same evidence of a shared genetic liability.
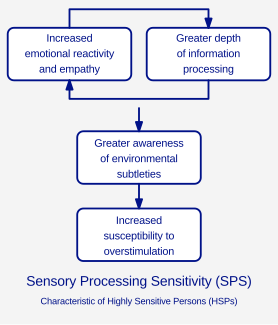
Sensory processing sensitivity (SPS) is a temperamental or personality trait involving "an increased sensitivity of the central nervous system and a deeper cognitive processing of physical, social and emotional stimuli". The trait is characterized by "a tendency to 'pause to check' in novel situations, greater sensitivity to subtle stimuli, and the engagement of deeper cognitive processing strategies for employing coping actions, all of which is driven by heightened emotional reactivity, both positive and negative".
Diagnoses of autism have become more frequent since the 1980s, which has led to various controversies about both the cause of autism and the nature of the diagnoses themselves. Whether autism has mainly a genetic or developmental cause, and the degree of coincidence between autism and intellectual disability, are all matters of current scientific controversy as well as inquiry. There is also more sociopolitical debate as to whether autism should be considered a disability on its own.
Autism spectrum disorder(ASD) is a developmental disorder that begins in early childhood, persists throughout adulthood, and affects three crucial areas of development: communication, social interaction and restricted patterns of behavior. There are many conditions comorbid to autism spectrum disorder such as fragile X syndrome and epilepsy.
Acute stress disorder is a psychological response to a terrifying, traumatic or surprising experience. It may bring about delayed stress reactions if not correctly addressed.
High-functioning autism (HFA) is an autism classification where a person exhibits no intellectual disability, but may exhibit deficits in communication, emotion recognition and expression, and social interaction. HFA is not included in either the American Psychological Association's DSM-5 or the World Health Organization's ICD-10, neither of which subdivides autism based on intellectual capabilities.
The following outline is provided as an overview of and topical guide to autism:
Developmental disability is a diverse group of chronic conditions that are due to mental or physical impairments that arise before adulthood. Developmental disabilities cause individuals living with them many difficulties in certain areas of life, especially in "language, mobility, learning, self-help, and independent living". Developmental disabilities can be detected early on and persist throughout an individual's lifespan. Developmental disability that affects all areas of a child's development is sometimes referred to as global developmental delay.

The University of North Carolina TEACCH Autism Program creates and disseminates community-based services, training programs, and research for individuals of all ages and skill levels with autism spectrum disorder (ASD), to enhance the quality of life for them and their families across the lifespan.

Sensory overload occurs when one or more of the body's senses experiences over-stimulation from the environment. There are many environmental elements that affect an individual. Examples of these elements are urbanization, crowding, noise, mass media, and technology.

Autism therapies include a wide variety of therapies that claim to help people with autism, or their families. Such methods of therapy also seek the increase of functional independence in autistic people. Many therapies marketed towards autistic people and/or their parents claim outcomes that have not been supported by Level of Research (LOE) Level 1 Level 1 research includes evidence from a systematic review or meta-analysis of all relevant RCTs or evidence-based clinical practice guidelines based on systematic reviews of RCTs or three or more RCTs of good quality that have similar results.
Social Stories were devised as a tool to help individuals with ASD better understand the nuances of interpersonal communication so that they could "interact in an effective and appropriate manner". Although the prescribed format was meant for high functioning people with basic communication skills, the format was adapted substantially to suit individuals with poor communication skills and low level functioning. The evidence shows that there has been minimal improvement in social interaction skills. However, it is difficult to assess whether the concept would have been successful if it had been carried out as designed.
Kanner autism, or classic autism, is an outdated neurodevelopmental diagnosis which is now considered part of autism spectrum disorder. The term 'autism' was historically used to refer specifically to classic autism, but it is now more commonly used for the spectrum at large.
Several factors complicate the diagnosis of Asperger syndrome (AS), an autism spectrum disorder (ASD). Like other ASD forms, Asperger syndrome is characterized by impairment in social interaction accompanied by restricted and repetitive interests and behavior; it differs from the other ASDs by having no general delay in language or cognitive development. Problems in diagnosis include disagreement among diagnostic criteria, the controversy over the distinction between AS and other ASD forms or even whether AS exists as a separate syndrome, and over- and under-diagnosis for non-technical reasons. As with other ASD forms, early diagnosis is important, and differential diagnosis must consider several other conditions.

The autism spectrum is a range of neurodevelopmental conditions generally characterized by difficulties in social interactions and communication, repetitive behaviors, intense interests, and unusual responses to sensory stimuli. It is commonly referred to as autism or, in the context of a professional diagnosis, as autism spectrum disorder (ASD), but the latter term remains controversial among neurodiversity advocates, neurodiversity researchers, and many autistic people due to the use of the word disorder and due to questions about its utility outside of diagnostic contexts.
Autism-friendly means being aware of social engagement and environmental factors affecting people on the autism spectrum, with modifications to communication methods and physical space to better suit individual's unique and special needs.
Low-functioning autism (LFA) is a degree of autism marked by difficulties with social communication and interaction, challenging behavior, and differences in social or emotional reciprocity. Sleep problems, aggression, stereotypical, and self-injurious behavior are also common symptoms. LFA is not a recognized diagnosis in the DSM-5 or ICD-10, as neither subdivides autism based on intellectual capabilities.

Sensory processing disorder (SPD) is a condition in which multisensory input is not adequately processed in order to provide appropriate responses to the demands of the environment. Sensory processing disorder is present in many with Autism spectrum disorders and Attention Deficit Hyperactivity Disorder. Individuals with SPD may inappropriately process visual, auditory, olfactory (smell), gustatory (taste), tactile (touch), vestibular (balance), proprioception, and interoception sensory stimuli.
Nonverbal autism is a subset of autism where the person does not learn how to speak. It is estimated that 25% to 50% of children diagnosed with autism spectrum disorder (ASD) never develop spoken language beyond a few words or utterances.
References
Notes
- 1 2 McDonnell, Reeves, Johnson & Lane, 1998, p. 164
- ↑ McDonnell, McEvoy & Dearden, (1994)
- ↑ McDonnell, (2010)
- ↑ Corbett, B.A. and Simon, D. (2013)
- ↑ Richetin, J. and Richardson, D.S. (2007)
- 1 2 McDonnell et al., (2015)
- ↑ Hutt, Hutt, Lee and Ounsted, 1964
- ↑ Althaus, van Roon, Mulder, Mulder, Aarnoudse and Minderaa 2004
- ↑ Hirstein Iversen and Ramachandran 2001
- ↑ van Engeland, Roelofs, Verbaten and Slangen, 1991
- ↑ Goodwin, et al., (2006)
- ↑ Hirstein, et al., (2001)
- 1 2 Rogers and Ozonoff, 2005
- ↑ Garey, Goodwillie, Frohlich, Morgan, Gustafsson, Smithies, Korach, Ogawa and Pfaff, 2003
- ↑ Rimland, 1964; DesLauriers and Carlson, 1969
- ↑ Kinsbourne, 1980
- ↑ Shore, 2003; O'Neill and Jones, 1997
- 1 2 3 Liss, Saulnier, Fein and Kinsbourne, 2006
- ↑ Howlin, 1998; Groden, Cautela, Prince and Berryman, 1994
- ↑ Lazarus and Folkman (1984)
- ↑ Frith, 2003
Resources
- Althaus, M.; van Roon, A.M.; Mulder, L.J.M.; Mulder, G.; Aarnoudse, C.C.; Minderaa, R.B. (2000). Autonomic Response Patterns Observed during the Performance of an attention Demanding Task in two groups of Children with Autistic-Type Difficulties in Social Adjustment. Psychophysiology, 41, 893–904.
- Corbett, B.A.; Simon, D. (2013). Adolescence, Stress and Cortisol in Autism Spectrum Disorders. Open Access Autism, 1(1), 2.
- Deslauriers, A.M.; Carlson, C.F. (1969). Your child is asleep: Early infantile autism. Homewood, IL: Dorsey Press;
- Frith, U. (2003). Autism Explaining the Enigma. (2nd Edition) Oxford: Blackwell.
- Garey, J.; Goodwillie, A.; Frohlich, J.; Morgan, M.; Gustaffson, J.A.; Smithies, O.; Korach, K.S.; Ogawa, S.; Pfaff, D.W. (2003) Genetic Contributions to Generalized Arousal of Brain and Behavior. Proceedings of the National Academy of Sciences of the United States of America, 100, 11019–11022.
- Goodwin, M.S.; Groden, J.; Velicer, W.F.; Lipsitt, L.P.; Grace Baron, M.; Hofmann, S.G.; Groden, G. (2006). Cardiovascular Arousal in Individuals With Autism. Focus on Autism and Other Developmental Disabilities, 21, 100–123.
- Groden, J.; Cautela, J.; Prince, S.; Berryman, J. (1994). The Impact of Stress and Anxiety on Individuals with Autism and other Developmental Disabilities. In E. Schopler and G. Mesibov (Eds.) Behavior Issues and Autism. New York, Plenum Publishing.
- Hirstein, W.; Iversen, P.; Ramachandran, V.S. (2001). Autonomic Responses of Autistic Children to People and Objects. Proceedings: Biological Sciences
- Howlin, P. (1998). Children with Autism and Aspergers Syndrome: A Guide for Practitioners and Carers. Chichester: Wiley.
- Hutt, C.; Hutt, S.J.; Lee, D.; Ounstead, C. (1964). Arousal and Childhood Autism. Nature, 204, 908–909.
- Kinsbourne, M. (1980). Do Repetitive Movement Patterns in Children and Animals Serve a Dearousing Function? Developmental and Behavioral Paediatrics, 1, 39–42.
- Lazarus, R.S.; Folkman, S. (1984). Stress, Appraisal, and Coping. New York: Springer.
- Liss, M.; Saulnier, C.; Fein, D; Kinsbourne, M. (2006). Sensory and Attention Abnormalities in Autistic Spectrum disorders. Autism, 10, 155–172
- McDonnell, A.A.; Waters, T.; Jones D. (2002). Low Arousal Approaches in the Management of Challenging Behaviours. In D. Allen (Ed) Ethical approaches to physical interventions: Responding to Challenging behaviours in people with Intellectual Disabilities. Plymouth: BILD, pp. 104–113.
- McDonnell, A.A.; McEvoy, J.; Dearden, R.L. (1994). Coping with Violent Situations in the Caring Environment. In T. Wykes (Ed) Violence and health care professionals. London: Chapman and Hall, pp. 189–206.
- McDonnell, A.A.; Reeves, S.; Johnson, A.; Lane, A. (1998). Management Challenging Behaviours in an Adult with Learning Disabilities: the Use of Low Arousal. Behavioural and Cognitive Psychotherapy, 26, 163–171.
- McDonnell, A.A. (2010). Managing Aggressive Behaviour in Care Settings: Understanding and Applying Low Arousal Approaches. Chichester: Wiley-Blackwell.
- McDonnell, A.A.; McCreadie, M.; Mills, R.; Deveau, R.; Anker, R.; Hayden, J. (2015). The Role of Physiological Arousal in the Management of Challenging Behaviours in Individuals with Autism Spectrum Disorders. Research in Developmental Disabilities, 36C, 311-322.
- McDonnell, A.A. (2019). The Reflective Journey: A Practitioner's Guide to the Low Arousal Approach. UK: Studio 3 Publications.
- O'Neill, M.; Jones, R.S.P. (1997). Sensory Perceptual Abnormalities in Autism: A Case for More Research. Journal of Autism and Developmental Disorders, 27(3), 283–293.
- Richetin, J.; Richardson, D.S. (2007). Automatic Processes and Individual Differences in Aggressive Behaviour. Aggression and Violent Behaviour, 13, 423-430.
- Rimland, B. (1964). Infantile autism, New York: Appleton Century Crofts.
- Rogers, S.J.; Ozonoff, S. (2005). What Do We Know About Sensory Dysfunction in Autism? A Critical Review of the Empirical Evidence. Journal of Child Psychology and Psychiatry, 46, 1255–1268.
- Shore S. (2003). Beyond the Wall: Personal Experiences with Autism and Asperger Syndrome: Autism Asperger publishing company.
- Van Engeland, H.; Roelofs, J.W.; Verbaten, M.N.; Slangen, J.L. (1991). Abnormal Electrodermal Reactivity to Novel Visual Stimuli in Autistic Children. Psychiatry Research, 38, 27–38.