
A cataract is a cloudy area in the lens of the eye that leads to a decrease in vision of the eye. Cataracts often develop slowly and can affect one or both eyes. Symptoms may include faded colours, blurry or double vision, halos around light, trouble with bright lights, and difficulty seeing at night. This may result in trouble driving, reading, or recognizing faces. Poor vision caused by cataracts may also result in an increased risk of falling and depression. Cataracts cause 51% of all cases of blindness and 33% of visual impairment worldwide.

Eye surgery, also known as ophthalmic surgery or ocular surgery, is surgery performed on the eye or its adnexa. Eye surgery is part of ophthalmology and is performed by an ophthalmologist or eye surgeon. The eye is a fragile organ, and requires due care before, during, and after a surgical procedure to minimize or prevent further damage. An eye surgeon is responsible for selecting the appropriate surgical procedure for the patient, and for taking the necessary safety precautions. Mentions of eye surgery can be found in several ancient texts dating back as early as 1800 BC, with cataract treatment starting in the fifth century BC. It continues to be a widely practiced class of surgery, with various techniques having been developed for treating eye problems.

Radial keratotomy (RK) is a refractive surgical procedure to correct myopia (nearsightedness). It was developed in 1974 by Svyatoslav Fyodorov, a Russian ophthalmologist. It has been largely supplanted by newer, more accurate operations, such as photorefractive keratectomy, LASIK, Epi-LASIK and the phakic intraocular lens.

Refractive surgery is optional eye surgery used to improve the refractive state of the eye and decrease or eliminate dependency on glasses or contact lenses. This can include various methods of surgical remodeling of the cornea (keratomileusis), lens implantation or lens replacement. The most common methods today use excimer lasers to reshape the curvature of the cornea. Refractive eye surgeries are used to treat common vision disorders such as myopia, hyperopia, presbyopia and astigmatism.

Phacoemulsification is a cataract surgery method in which the internal lens of the eye which has developed a cataract is emulsified with the tip of an ultrasonic handpiece and aspirated from the eye. Aspirated fluids are replaced with irrigation of balanced salt solution to maintain the volume of the anterior chamber during the procedure. This procedure minimises the incision size and reduces the recovery time and risk of surgery induced astigmatism.

An Intraocular lens (IOL) is a lens implanted in the eye usually as part of a treatment for cataracts or for correcting other vision problems such as short sightedness and long sightedness; a form of refractive surgery. If the natural lens is left in the eye, the IOL is known as phakic, otherwise it is a pseudophakic lens. Both kinds of IOLs are designed to provide the same light-focusing function as the natural crystalline lens. This can be an alternative to LASIK, but LASIK is not an alternative to an IOL for treatment of cataracts.

A phakic intraocular lens (PIOL) is an intraocular lens that is implanted surgically into the eye to correct refractive errors without removing the natural lens. Intraocular lenses that are implanted into eyes after the eye's natural lens has been removed during cataract surgery are known as pseudophakic.
Cataract surgery, also called lens replacement surgery, is the removal of the natural lens of the eye that has developed a cataract, an opaque or cloudy area. The eye's natural lens is usually replaced with an artificial intraocular lens (IOL) implant.
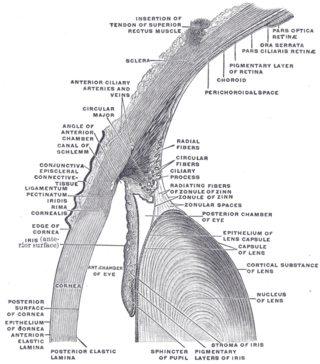
The lens capsule is a component of the globe of the eye. It is a clear elastic basement membrane similar in composition to other basement membranes in the body. The capsule is very thick basement membraneand the thickness varies in different areas on the lens surface and with the age of the animal. It and is composed of various types of fibers such as collagen IV laminin etc. and these help it stay under constant tension. The capsule is attached to the surrounding eye by numerous suspensory ligaments and in turn suspends the rest of the lens in an appropriate position. As the lens grows throughout life so must the capsule. Due to the shape of the capsule the lens naturally tends towards a rounder or more globular configuration, a shape it must assume for the eye to focus at a near distance. Tension on the capsule is varied to allow the lens to subtly change shape to allow the eye to focus in a process called accommodation.

Astigmatism is a type of refractive error due to rotational asymmetry in the eye's refractive power. This results in distorted or blurred vision at any distance. Other symptoms can include eyestrain, headaches, and trouble driving at night. Astigmatism often occurs at birth and can change or develop later in life. If it occurs in early life and is left untreated, it may result in amblyopia.
Howard V. Gimbel FRCSC, AOE, FACS, CABES, is a Canadian ophthalmologist, university professor, senior editor, and amateur musician. He is better known for his invention, along with Thomas Neuhann, of the continuous curvilinear capsulorhexis (CCC), a technique employed in modern cataract surgery.

Capsulotomy is a type of eye surgery in which an incision is made into the capsule of the crystalline lens of the eye. In modern cataract operations, the lens capsule is usually not removed. The most common forms of cataract surgery remove nearly all of the crystalline lens but do not remove the crystalline lens capsule. The crystalline lens capsule is retained and used to contain and position the intraocular lens implant (IOL).
The aim of an accurate intraocular lens power calculation is to provide an intraocular lens (IOL) that fits the specific needs and desires of the individual patient. The development of better instrumentation for measuring the eye's axial length (AL) and the use of more precise mathematical formulas to perform the appropriate calculations have significantly improved the accuracy with which the surgeon determines the IOL power.
David J. Apple was an ophthalmic pathologist who conducted research on the pathology of intraocular lens complications as well as ophthalmic surgery in general. He was a medical historian and biographer of Sir Harold Ridley, the inventor of the intraocular lens (IOL).
He often stated that Harold Ridley changed the world. What we can say about David Apple is that he vastly improved the world that Harold Ridley changed
Dr Amar Agarwal M.S., FRCS, F.R.C.Ophth is an Indian ophthalmologist and chairman and managing director of Dr. Agarwal's Eye Hospital and Eye Research Centre in India, which includes 140+ eye hospitals. He is the recipient of the Best Doctor award of the State government from then Chief Minister of Tamil Nadu J Jayalalithaa on 15 August 2014. He is also the past President of the International Society of Refractive Surgery (ISRS) and Secretary General of the Intraocular Implant and Refractive Society of India (IIRSI).

In ophthalmology, glued intraocular lens or glued IOL is a surgical technique for implantation, with the use of biological glue, of a posterior chamber IOL in eyes with deficient or absent posterior capsules. A quick-acting surgical fibrin sealant derived from human blood plasma, with both hemostatic and adhesive properties, is used.
Intraocular lens scaffold, or IOL scaffold technique, is a surgical procedure in ophthalmology. In cases where the posterior lens capsule is ruptured and the cataract is present, an intraocular lens (IOL) can be inserted under the cataract. The IOL acts as a scaffold, and prevents the cataract pieces from falling to the back of the eye. The cataract can then be safely removed by emulsifying it with ultrasound and aspiration. This technique is called IOL scaffold, and was initiated by Amar Agarwal at Dr. Agarwal's Eye Hospital in Chennai, India.

Phacolytic glaucoma (PG) is a form of glaucoma which is caused due to a leaking mature or immature cataract. Inflammatory glaucoma which occurs in phacolysis is a condition which is a result of the leakage of protein within the lens into the capsule of a mature or hyper mature cataract and involves a simple procedure to be cured that is referred to as cataract extraction.
Clear lens extraction (CLE), also known as refractive lensectomy, custom lens replacement (CLR) or refractive lens exchange (RLE) is a surgical procedure in which clear lens of the human eye is removed. Unlike cataract surgery, where cloudy lens is removed to treat cataract, clear lens extraction is done to surgically correct refractive errors such as high myopia. It can also be done in hyperopic or presbyopic patients who wish to have a multifocal IOL implanted to avoid wearing glasses. It is also used as a treatment for diseases such as angle closure glaucoma.
Cataract surgery has a long history in Europe, Asia, and Africa. It is one of the most common and successful surgical procedures in worldwide use, thanks to improvements in techniques for cataract removal and developments in intraocular lens (IOL) replacement technology, in implantation techniques, and in IOL design, construction, and selection. Surgical techniques that have contributed to this success include microsurgery, viscoelastics, and phacoemulsification.
