
Diabetic retinopathy, is a medical condition in which damage occurs to the retina due to diabetes. It is a leading cause of blindness in developed countries.

A cataract is a cloudy area in the lens of the eye that leads to a decrease in vision of the eye. Cataracts often develop slowly and can affect one or both eyes. Symptoms may include faded colours, blurry or double vision, halos around light, trouble with bright lights, and difficulty seeing at night. This may result in trouble driving, reading, or recognizing faces. Poor vision caused by cataracts may also result in an increased risk of falling and depression. Cataracts cause 51% of all cases of blindness and 33% of visual impairment worldwide.

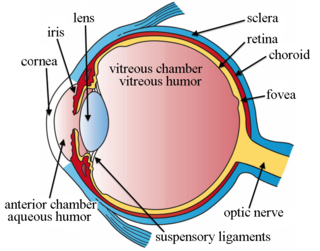
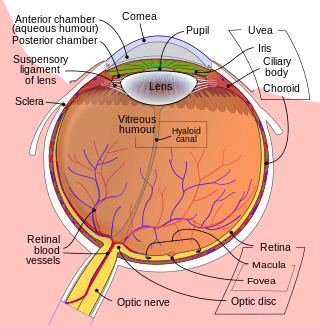
Floaters or eye floaters are sometimes visible deposits within the eye's vitreous humour, which is normally transparent, or between the vitreous and retina. They can become particularly noticeable when looking at a blank surface or an open monochromatic space, such as blue sky. Each floater can be measured by its size, shape, consistency, refractive index, and motility. They are also called muscae volitantes, or mouches volantes. The vitreous usually starts out transparent, but imperfections may gradually develop as one ages. The common type of floater, present in most people's eyes, is due to these degenerative changes of the vitreous. The perception of floaters, which may be annoying or problematic to some people, is known as myodesopsia, or, less commonly, as myodaeopsia, myiodeopsia, or myiodesopsia. It is not often treated, except in severe cases, where vitrectomy (surgery), laser vitreolysis, and medication may be effective.

Vitrectomy is a surgery to remove some or all of the vitreous humor from the eye.

Phacoemulsification is a cataract surgery method in which the internal lens of the eye which has developed a cataract is emulsified with the tip of an ultrasonic handpiece and aspirated from the eye. Aspirated fluids are replaced with irrigation of balanced salt solution to maintain the volume of the anterior chamber during the procedure. This procedure minimises the incision size and reduces the recovery time and risk of surgery induced astigmatism.

Retinal detachment is a disorder of the eye in which the retina peels away from its underlying layer of support tissue. Initial detachment may be localized, but without rapid treatment the entire retina may detach, leading to vision loss and blindness. It is a surgical emergency.

Cefuroxime, sold under the brand name Zinacef among others, is a second-generation cephalosporin antibiotic used to treat and prevent a number of bacterial infections. These include pneumonia, meningitis, otitis media, sepsis, urinary tract infections, and Lyme disease. It is used by mouth or by injection into a vein or muscle.
Cataract surgery, also called lens replacement surgery, is the removal of the natural lens of the eye that has developed a cataract, an opaque or cloudy area. The eye's natural lens is usually replaced with an artificial intraocular lens (IOL) implant.

Physical or chemical injuries of the eye can be a serious threat to vision if not treated appropriately and in a timely fashion. The most obvious presentation of ocular (eye) injuries is redness and pain of the affected eyes. This is not, however, universally true, as tiny metallic projectiles may cause neither symptom. Tiny metallic projectiles should be suspected when a patient reports metal on metal contact, such as with hammering a metal surface. Corneal foreign bodies are one of the most common preventable occupational hazards. Intraocular foreign bodies do not cause pain because of the lack of nerve endings in the vitreous humour and retina that can transmit pain sensations. As such, general or emergency department doctors should refer cases involving the posterior segment of the eye or intraocular foreign bodies to an ophthalmologist. Ideally, ointment would not be used when referring to an ophthalmologist, since it diminishes the ability to carry out a thorough eye examination.
Staphylococcus lugdunensis is a coagulase-negative member of the genus Staphylococcus, consisting of Gram-positive bacteria with spherical cells that appear in clusters.
Intravitreal administration is a route of administration of a drug, or other substance, in which the substance is delivered into the vitreous humor of the eye. "Intravitreal" literally means "inside an eye". Intravitreal injections were first introduced in 1911 when Ohm gave an injection of air into the vitreous humor to repair a detached retina. In the mid-1940s, intravitreal injections became a standard way to administer drugs to treat endophthalmitis and cytomegalovirus retinitis.
Intermediate uveitis is a form of uveitis localized to the vitreous and peripheral retina. Primary sites of inflammation include the vitreous of which other such entities as pars planitis, posterior cyclitis, and hyalitis are encompassed. Intermediate uveitis may either be an isolated eye disease or associated with the development of a systemic disease such as multiple sclerosis or sarcoidosis. As such, intermediate uveitis may be the first expression of a systemic condition. Infectious causes of intermediate uveitis include Epstein–Barr virus infection, Lyme disease, HTLV-1 virus infection, cat scratch disease, and hepatitis C.

Branch retinal vein occlusion is a common retinal vascular disease of the elderly. It is caused by the occlusion of one of the branches of central retinal vein.
Vitreomacular adhesion (VMA) is a human medical condition where the vitreous gel of the human eye adheres to the retina in an abnormally strong manner. As the eye ages, it is common for the vitreous to separate from the retina. But if this separation is not complete, i.e. there is still an adhesion, this can create pulling forces on the retina that may result in subsequent loss or distortion of vision. The adhesion in of itself is not dangerous, but the resulting pathological vitreomacular traction (VMT) can cause severe ocular damage.
Open-globe injuries are full-thickness eye-wall wounds requiring urgent diagnosis and treatment.
An intracameral injection is usually of an antibiotic into the anterior chamber of the eyeball to prevent endophthalmitis caused by an infection of the eye that can occur after cataract surgery. The Food and Drug Administration (FDA) has not approved antibiotics for this use and it is considered 'off-label'. Concerns about this procedure contributing to increasing numbers of antibiotic resistant bacteria have been expressed.
Intravitreal injection is the method of administration of drugs into the eye by injection with a fine needle. The medication will be directly applied into the vitreous humor. It is used to treat various eye diseases, such as age-related macular degeneration (AMD), diabetic retinopathy, and infections inside the eye such as endophthalmitis. As compared to topical administration, this method is beneficial for a more localized delivery of medications to the targeted site, as the needle can directly pass through the anatomical eye barrier and dynamic barrier. It could also minimize adverse drug effects on other body tissues via the systemic circulation, which could be a possible risk for intravenous injection of medications. Although there are risks of infections or other complications, with suitable precautions throughout the injection process, chances for these complications could be lowered.

Secondary glaucoma is a collection of progressive optic nerve disorders associated with a rise in intraocular pressure (IOP) which results in the loss of vision. In clinical settings, it is defined as the occurrence of IOP above 21 mmHg requiring the prescription of IOP-managing drugs. It can be broadly divided into two subtypes: secondary open-angle glaucoma and secondary angle-closure glaucoma, depending on the closure of the angle between the cornea and the iris. Principal causes of secondary glaucoma include optic nerve trauma or damage, eye disease, surgery, neovascularization, tumours and use of steroid and sulfa drugs. Risk factors for secondary glaucoma include uveitis, cataract surgery and also intraocular tumours. Common treatments are designed according to the type and the underlying causative condition, in addition to the consequent rise in IOP. These include drug therapy, the use of miotics, surgery or laser therapy.
Panuveitis also known as Diffuse uveitis or Total uveitis is an eye disease affecting the internal structures of the eye. In this inflammation occurs throughout the uveal tract, with no specific areas of predominant inflammation. In most cases, along with the uvea, the retina, vitreous humor, optic nerve or lens are also involved.
Manual small incision cataract surgery (MSICS) is an evolution of extracapsular cataract extraction (ECCE); the lens is removed from the eye through a self-sealing scleral tunnel wound. A well-constructed scleral tunnel is held closed by internal pressure, is watertight, and does not require suturing. The wound is relatively smaller than that in ECCE but is still markedly larger than a phacoemulsification wound. Comparative trials of MSICS against phaco in dense cataracts have found no statistically significant difference in outcomes but MSICS had shorter operating times and significantly lower costs. MSICS has become the method of choice in the developing world because it provides high-quality outcomes with less surgically induced astigmatism than ECCE, no suture-related problems, quick rehabilitation, and fewer post-operative visits. MSICS is easy and fast to learn for the surgeon, cost effective, simple, and applicable to almost all types of cataract.
