Intravenous therapy is a medical technique that administers fluids, medications and nutrients directly into a person's vein. The intravenous route of administration is commonly used for rehydration or to provide nutrients for those who cannot, or will not—due to reduced mental states or otherwise—consume food or water by mouth. It may also be used to administer medications or other medical therapy such as blood products or electrolytes to correct electrolyte imbalances. Attempts at providing intravenous therapy have been recorded as early as the 1400s, but the practice did not become widespread until the 1900s after the development of techniques for safe, effective use.
Thrombosis is the formation of a blood clot inside a blood vessel, obstructing the flow of blood through the circulatory system. When a blood vessel is injured, the body uses platelets (thrombocytes) and fibrin to form a blood clot to prevent blood loss. Even when a blood vessel is not injured, blood clots may form in the body under certain conditions. A clot, or a piece of the clot, that breaks free and begins to travel around the body is known as an embolus.

Venous thrombosis is the blockage of a vein caused by a thrombus. A common form of venous thrombosis is deep vein thrombosis (DVT), when a blood clot forms in the deep veins. If a thrombus breaks off (embolizes) and flows to the lungs to lodge there, it becomes a pulmonary embolism (PE), a blood clot in the lungs. The conditions of DVT only, DVT with PE, and PE only, are all captured by the term venous thromboembolism (VTE).

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.
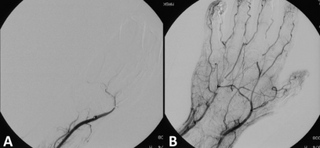
Thrombolysis, also called fibrinolytic therapy, is the breakdown (lysis) of blood clots formed in blood vessels, using medication. It is used in ST elevation myocardial infarction, stroke, and in cases of severe venous thromboembolism.
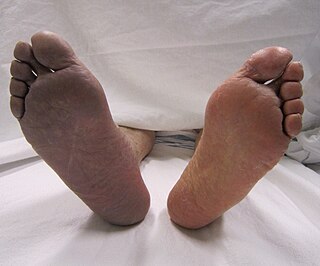
Deep vein thrombosis (DVT) is a type of venous thrombosis involving the formation of a blood clot in a deep vein, most commonly in the legs or pelvis. A minority of DVTs occur in the arms. Symptoms can include pain, swelling, redness, and enlarged veins in the affected area, but some DVTs have no symptoms.
A pseudoaneurysm, also known as a false aneurysm, is a locally contained hematoma outside an artery or the heart due to damage to the vessel wall. The injury passes through all three layers of the arterial wall, causing a leak, which is contained by a new, weak "wall" formed by the products of the clotting cascade. A pseudoaneurysm does not contain any layer of the vessel wall.

A dialysis catheter is a catheter used for exchanging blood to and from a hemodialysis machine and a patient.

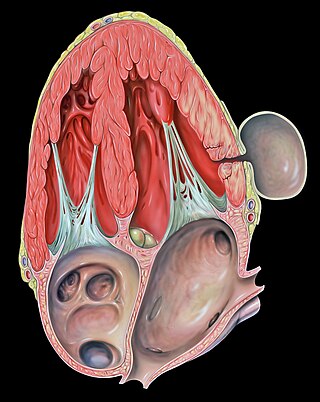
A pulmonary artery catheter (PAC), also known as a Swan-Ganz catheter or right heart catheter, is a balloon-tipped catheter that is inserted into a pulmonary artery in a procedure known as pulmonary artery catheterization or right heart catheterization. Pulmonary artery catheterization is a useful measure of the overall function of the heart particularly in those with complications from heart failure, heart attack, arrythmias or pulmonary embolism. It is also a good measure for those needing intravenous fluid therapy, for instance post heart surgery, shock, and severe burns. The procedure can also be used to measure pressures in the heart chambers.

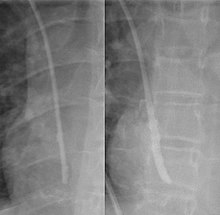
A peripherally inserted central catheter, less commonly called a percutaneous indwelling central catheter, is a form of intravenous access that can be used for a prolonged period of time or for administration of substances that should not be done peripherally. It is a catheter that enters the body through the skin (percutaneously) at a peripheral site, extends to the superior vena cava, and stays in place for days, weeks or even months.

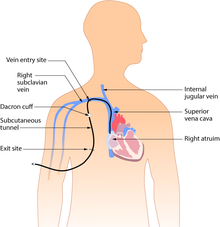
A Hickman line is a central venous catheter most often used for the administration of chemotherapy or other medications, as well as for the withdrawal of blood for analysis. Some types are used mainly for the purpose of apheresis or dialysis. They have also been used in total parenteral nutrition (TPN). Hickman lines may remain in place for extended periods and are used when long-term intravenous access is required.
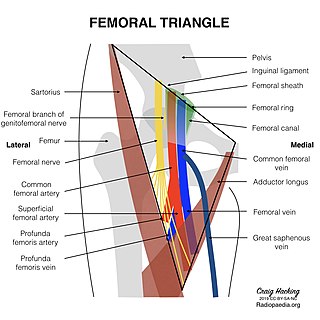
In the human body, the femoral vein is the vein that accompanies the femoral artery in the femoral sheath. It is a deep vein that begins at the adductor hiatus as the continuation of the popliteal vein. The great saphenous vein, and the deep femoral vein drain into the femoral vein in the femoral triangle when it becomes known as the common femoral vein. It ends at the inferior margin of the inguinal ligament where it becomes the external iliac vein. Its major tributaries are the deep femoral vein, and the great saphenous vein. The femoral vein contains valves.

Renal vein thrombosis (RVT) is the formation of a clot in the vein that drains blood from the kidneys, ultimately leading to a reduction in the drainage of one or both kidneys and the possible migration of the clot to other parts of the body. First described by German pathologist Friedrich Daniel von Recklinghausen in 1861, RVT most commonly affects two subpopulations: newly born infants with blood clotting abnormalities or dehydration and adults with nephrotic syndrome.
Vascular access refers to a rapid, direct method of introducing or removing devices or chemicals from the bloodstream. In hemodialysis, vascular access is used to remove the patient's blood so that it can be filtered through the dialyzer. Three primary methods are used to gain access to the blood: an intravenous catheter, an arteriovenous fistula (AV) or a synthetic graft. In the latter two, needles are used to puncture the graft or fistula each time dialysis is performed.

An umbilical line is a catheter that is inserted into one of the two arteries or the vein of the umbilical cord. Generally the UAC/UVC is used in Neonatal Intensive Care Units (NICU) as it provides quick access to the central circulation of premature infants. UAC/UVC lines can be placed at the time of birth and allow medical staff to quickly infuse fluids, inotropic drugs, and blood if required. It is sometimes used in term or near-term newborns in whom the umbilical cord stump is still connected to the circulatory system. Medications, fluids, and blood can be given through this catheter and it allows monitoring of blood gasses and withdrawing of blood samples. Transumbilical catheter intervention is also a method of gaining access to the heart, for example to surgically correct a patent ductus arteriosus.

In medicine, a port is a small medical appliance that is installed beneath the skin. A catheter connects the port to a vein. Under the skin, the port has a septum through which drugs can be injected and blood samples can be drawn many times, usually with less discomfort for the patient than a more typical "needle stick".

In medicine, a peripheral venous catheter, peripheral venous line, peripheral venous access catheter, or peripheral intravenous catheter, is a catheter placed into a peripheral vein for venous access to administer intravenous therapy such as medication fluids.

Arterial embolism is a sudden interruption of blood flow to an organ or body part due to an embolus adhering to the wall of an artery blocking the flow of blood, the major type of embolus being a blood clot (thromboembolism). Sometimes, pulmonary embolism is classified as arterial embolism as well, in the sense that the clot follows the pulmonary artery carrying deoxygenated blood away from the heart. However, pulmonary embolism is generally classified as a form of venous embolism, because the embolus forms in veins. Arterial embolism is the major cause of infarction.
Venous access is any method used to access the bloodstream through the veins, either to administer intravenous therapy, parenteral nutrition, to obtain blood for analysis, or to provide an access point for blood-based treatments such as dialysis or apheresis. Access is most commonly achieved via the Seldinger technique, and guidance tools such as ultrasound and fluoroscopy can also be used to assist with visualizing access placement.
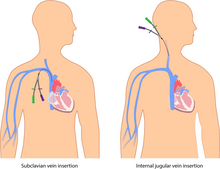
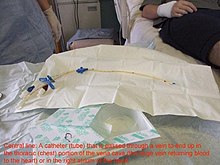
In medicine, vascular access is a means of accessing the bloodstream through the peripheral or central blood vessels in order to obtain blood or deliver medications including chemotherapy. A vascular access procedure involves insertion of a sterile plastic tube called a catheter into a blood vessel. Types of catheters can be either peripherally or centrally located. Peripheral catheters are approximately one inch (25 mm) long and are inserted into the small veins of the forearm. Central catheters are bigger and longer and are inserted into the large veins of the extremities, neck, or chest. Central venous catheters are the primary modality used for delivery of chemotherapeutic agents. The duration of central venous catheterization is dependent on the type of treatment given.