
Waterhouse–Friderichsen syndrome (WFS) is defined as adrenal gland failure due to bleeding into the adrenal glands, commonly caused by severe bacterial infection. Typically, it is caused by Neisseria meningitidis.

Shock is the state of insufficient blood flow to the tissues of the body as a result of problems with the circulatory system. Initial symptoms of shock may include weakness, fast heart rate, fast breathing, sweating, anxiety, and increased thirst. This may be followed by confusion, unconsciousness, or cardiac arrest, as complications worsen.

Sepsis is a potentially life-threatening condition that arises when the body's response to infection causes injury to its own tissues and organs.

Toxic shock syndrome (TSS) is a condition caused by bacterial toxins. Symptoms may include fever, rash, skin peeling, and low blood pressure. There may also be symptoms related to the specific underlying infection such as mastitis, osteomyelitis, necrotising fasciitis, or pneumonia.
Bloodstream infections (BSIs) are infections of blood caused by blood-borne pathogens. Blood is normally a sterile environment, so the detection of microbes in the blood is always abnormal. A bloodstream infection is different from sepsis, which is characterized by severe inflammatory or immune responses of the host organism to pathogens.
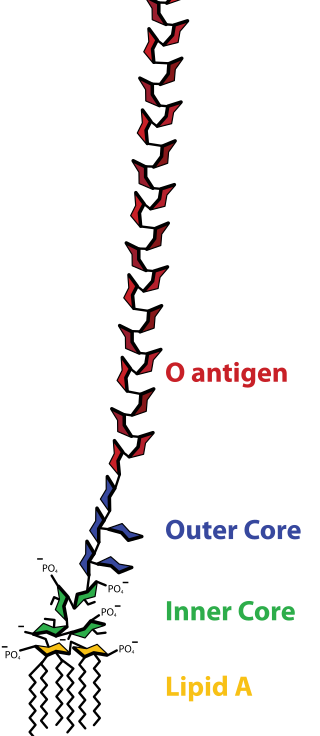
Lipopolysaccharides (LPS) are large molecules consisting of a lipid and a polysaccharide that are bacterial toxins. They are composed of an O-antigen, an outer core, and an inner core all joined by covalent bonds, and are found in the bacterial capsule, the outermost membrane of cell envelope of Gram-negative bacteria, such as E. coli and Salmonella. Today, the term endotoxin is often used synonymously with LPS, although there are a few endotoxins that are not related to LPS, such as the so-called delta endotoxin proteins produced by Bacillus thuringiensis.
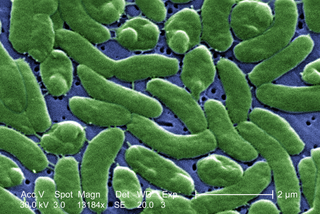
Vibrio vulnificus is a species of Gram-negative, motile, curved rod-shaped (vibrio), pathogenic bacteria of the genus Vibrio. Present in marine environments such as estuaries, brackish ponds, or coastal areas, V. vulnificus is related to V. cholerae, the causative agent of cholera. At least one strain of V. vulnificus is bioluminescent. Increasing seasonal ocean temperatures and low-salt marine environments like estuaries favor a greater concentration of Vibrio within filter-feeding shellfish; V. vulnificus infections in the Eastern United States have increased eightfold from 1988–2018.
In immunology, systemic inflammatory response syndrome (SIRS) is an inflammatory state affecting the whole body. It is the body's response to an infectious or noninfectious insult. Although the definition of SIRS refers to it as an "inflammatory" response, it actually has pro- and anti-inflammatory components.
Multiple organ dysfunction syndrome (MODS) is altered organ function in an acutely ill patient requiring medical intervention to achieve homeostasis.
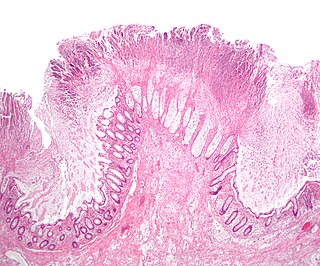
Toxic megacolon is an acute form of colonic distension. It is characterized by a very dilated colon (megacolon), accompanied by abdominal distension (bloating), and sometimes fever, abdominal pain, or shock.

Gas gangrene is a bacterial infection that produces tissue gas in gangrene. This deadly form of gangrene usually is caused by Clostridium perfringens bacteria. About 1,000 cases of gas gangrene are reported yearly in the United States.
Community-acquired pneumonia (CAP) refers to pneumonia contracted by a person outside of the healthcare system. In contrast, hospital-acquired pneumonia (HAP) is seen in patients who have recently visited a hospital or who live in long-term care facilities. CAP is common, affecting people of all ages, and its symptoms occur as a result of oxygen-absorbing areas of the lung (alveoli) filling with fluid. This inhibits lung function, causing dyspnea, fever, chest pains and cough.
Distributive shock is a medical condition in which abnormal distribution of blood flow in the smallest blood vessels results in inadequate supply of blood to the body's tissues and organs. It is one of four categories of shock, a condition where there is not enough oxygen-carrying blood to meet the metabolic needs of the cells which make up the body's tissues and organs. Distributive shock is different from the other three categories of shock in that it occurs even though the output of the heart is at or above a normal level. The most common cause is sepsis leading to a type of distributive shock called septic shock, a condition that can be fatal.

A Jarisch–Herxheimer reaction is a sudden and typically transient reaction that may occur within 24 hours of being administered antibiotics for an infection by a spirochete, including syphilis, leptospirosis, Lyme disease, and relapsing fever. Signs and symptoms include fever, chills, shivers, feeling sick, headache, fast heart beat, low blood pressure, breathing fast, flushing of skin, muscle aches, and worsening of skin lesions. It may sometimes be mistaken as an allergy to the antibiotic.
End organ damage is severe impairment of major body organs due to high blood pressure or states of low blood pressure or low blood volume. This can present as a heart attack or heart failure, pulmonary edema, neurologic deficits including a stroke, or acute kidney failure.
Capillary leak syndrome, or vascular leak syndrome, is characterized by the escape of blood plasma through capillary walls, from the blood circulatory system to surrounding tissues, muscle compartments, organs or body cavities. It is a phenomenon most commonly witnessed in sepsis, and less frequently in autoimmune diseases, differentiation syndrome, engraftment syndrome, hemophagocytic lymphohistiocytosis, the ovarian hyperstimulation syndrome, viral hemorrhagic fevers, and snakebite and ricin poisoning. Pharmaceuticals, including the chemotherapy medications gemcitabine and denileukin diftitox, as well as certain interleukins and monoclonal antibodies, can also cause capillary leaks. These conditions and factors are sources of secondary capillary leak syndrome.
Critical illness–related corticosteroid insufficiency is a form of adrenal insufficiency in critically ill patients who have blood corticosteroid levels which are inadequate for the severe stress response they experience. Combined with decreased glucocorticoid receptor sensitivity and tissue response to corticosteroids, this adrenal insufficiency constitutes a negative prognostic factor for intensive care patients.
Septic abortion describes any type of abortion, due to an upper genital tract bacterial infection including the inflammation of the endometrium during or after 20 weeks of gestation. The genital tract during this period is particularly vulnerable to infection, and sepsis in most cases is caused by a combination of factors both due to facility conditions and/or individual predispositions. The infection often starts in the placenta and fetus, with a potential complication of also affecting the uterus, that can result in sepsis spreading to surrounding organs, or pelvic infections.

Norepinephrine, also known as noradrenaline, is a medication used to treat people with very low blood pressure. It is the typical medication used in sepsis if low blood pressure does not improve following intravenous fluids. It is the same molecule as the hormone and neurotransmitter norepinephrine. It is given by slow injection into a vein.
Vasodilatory shock, vasogenic shock, or vasoplegic shock is a medical emergency belonging to shock along with cardiogenic shock, septic shock, allergen-induced shock and hypovolemic shock. When the blood vessels suddenly relax, it results in vasodilation. In vasodilatory shock, the blood vessels are too relaxed leading to extreme vasodilation and blood pressure drops and blood flow becomes very low. Without enough blood pressure, blood and oxygen will not be pushed to reach the body's organs. If vasodilatory shock lasts more than a few minutes, the lack of oxygen starts to damage the body's organs. Vasodilatory shock like other types of shock should be treated quickly, otherwise it can cause permanent organ damage or death as a result of multiple organ dysfunction.

