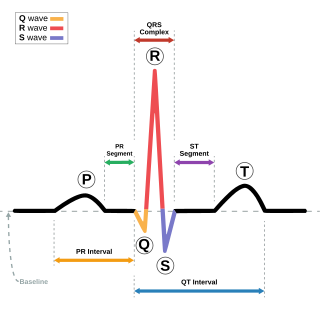
Electrocardiography is the process of producing an electrocardiogram, a recording of the heart's electrical activity through repeated cardiac cycles. It is an electrogram of the heart which is a graph of voltage versus time of the electrical activity of the heart using electrodes placed on the skin. These electrodes detect the small electrical changes that are a consequence of cardiac muscle depolarization followed by repolarization during each cardiac cycle (heartbeat). Changes in the normal ECG pattern occur in numerous cardiac abnormalities, including:

Tachycardia, also called tachyarrhythmia, is a heart rate that exceeds the normal resting rate. In general, a resting heart rate over 100 beats per minute is accepted as tachycardia in adults. Heart rates above the resting rate may be normal or abnormal.

Sinus node dysfunction (SND), also known as sick sinus syndrome (SSS), is a group of abnormal heart rhythms (arrhythmias) usually caused by a malfunction of the sinus node, the heart's primary pacemaker. Tachycardia-bradycardia syndrome is a variant of sick sinus syndrome in which the arrhythmia alternates between fast and slow heart rates.

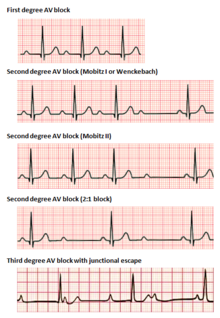
Third-degree atrioventricular block is a medical condition in which the electrical impulse generated in the sinoatrial node in the atrium of the heart can not propagate to the ventricles.

The cardiac conduction system transmits the signals generated by the sinoatrial node – the heart's pacemaker, to cause the heart muscle to contract, and pump blood through the body's circulatory system. The pacemaking signal travels through the right atrium to the atrioventricular node, along the bundle of His, and through the bundle branches to Purkinje fibers in the walls of the ventricles. The Purkinje fibers transmit the signals more rapidly to stimulate contraction of the ventricles.

Second-degree atrioventricular block is a disease of the electrical conduction system of the heart. It is a conduction block between the atria and ventricles. The presence of second-degree AV block is diagnosed when one or more of the atrial impulses fail to conduct to the ventricles due to impaired conduction. It is classified as a block of the AV node, falling between first-degree and third degree blocks.

Supraventricular tachycardia (SVT) is an umbrella term for fast heart rhythms arising from the upper part of the heart. This is in contrast to the other group of fast heart rhythms – ventricular tachycardia, which start within the lower chambers of the heart. There are four main types of SVT: atrial fibrillation, atrial flutter, paroxysmal supraventricular tachycardia (PSVT), and Wolff–Parkinson–White syndrome. The symptoms of SVT include palpitations, feeling of faintness, sweating, shortness of breath, and/or chest pain.
A junctional escape beat is a delayed heartbeat originating not from the atrium but from an ectopic focus somewhere in the atrioventricular junction. It occurs when the rate of depolarization of the sinoatrial node falls below the rate of the atrioventricular node. This dysrhythmia also may occur when the electrical impulses from the SA node fail to reach the AV node because of SA or AV block. It is a protective mechanism for the heart, to compensate for the SA node no longer handling the pacemaking activity, and is one of a series of backup sites that can take over pacemaker function when the SA node fails to do so. It can also occur following a premature ventricular contraction or blocked premature atrial contraction.

Atrioventricular block is a type of heart block that occurs when the electrical signal traveling from the atria, or the upper chambers of the heart, to ventricles, or the lower chambers of the heart, is impaired. Normally, the sinoatrial node produces an electrical signal to control the heart rate. The signal travels from the SA node to the ventricles through the atrioventricular node. In an AV block, this electrical signal is either delayed or completely blocked. When the signal is completely blocked, the ventricles produce their own electrical signal to control the heart rate. The heart rate produced by the ventricles is much slower than that produced by the SA node.
Premature atrial contraction (PAC), also known as atrial premature complexes (APC) or atrial premature beats (APB), are a common cardiac dysrhythmia characterized by premature heartbeats originating in the atria. While the sinoatrial node typically regulates the heartbeat during normal sinus rhythm, PACs occur when another region of the atria depolarizes before the sinoatrial node and thus triggers a premature heartbeat, in contrast to escape beats, in which the normal sinoatrial node fails, leaving a non-nodal pacemaker to initiate a late beat.

In cardiology, a ventricular escape beat is a self-generated electrical discharge initiated by, and causing contraction of the ventricles of the heart; normally the heart rhythm is begun in the atria of the heart and is subsequently transmitted to the ventricles. The ventricular escape beat follows a long pause in ventricular rhythm and acts to prevent cardiac arrest. It indicates a failure of the electrical conduction system of the heart to stimulate the ventricles.

Multifocal atrial tachycardia (MAT) is an abnormal heart rhythm, specifically a type of supraventricular tachycardia, that is particularly common in older people and is associated with exacerbations of chronic obstructive pulmonary disease (COPD). Normally, the heart rate is controlled by a cluster of cells called the sinoatrial node. When a number of different clusters of cells outside the SA node take over control of the heart rate, and the rate exceeds 100 beats per minute, this is called multifocal atrial tachycardia.
Sinoatrial arrest is a medical condition wherein the sinoatrial node of the heart transiently ceases to generate the electrical impulses that normally stimulate the myocardial tissues to contract and thus the heart to beat. It is defined as lasting from 2.0 seconds to several minutes. Since the heart contains multiple pacemakers, this interruption of the cardiac cycle generally lasts only a few seconds before another part of the heart, such as the atrio-ventricular junction or the ventricles, begins pacing and restores the heart action. This condition can be detected on an electrocardiogram (ECG) as a brief period of irregular length with no electrical activity before either the sinoatrial node resumes normal pacing, or another pacemaker begins pacing. If a pacemaker other than the sinoatrial node is pacing the heart, this condition is known as an escape rhythm. If no other pacemaker begins pacing during an episode of sinus arrest it becomes a cardiac arrest. This condition is sometimes confused with sinoatrial block, a condition in which the pacing impulse is generated, but fails to conduct through the myocardium. Differential diagnosis of the two conditions is possible by examining the exact length of the interruption of cardiac activity. If the next available pacemaker takes over, it is in the following order:

Accelerated idioventricular rhythm is a ventricular rhythm with a rate of between 40 and 120 beats per minute. Idioventricular means “relating to or affecting the cardiac ventricle alone” and refers to any ectopic ventricular arrhythmia. Accelerated idioventricular arrhythmias are distinguished from ventricular rhythms with rates less than 40 and those faster than 120. Though some other references limit to between 60 and 100 beats per minute. It is also referred to as AIVR and "slow ventricular tachycardia."

Junctional rhythm also called nodal rhythm describes an abnormal heart rhythm resulting from impulses coming from a locus of tissue in the area of the atrioventricular node, the "junction" between atria and ventricles.

A sinoatrial block is a disorder in the normal rhythm of the heart, known as a heart block, that is initiated in the sinoatrial node. The initial action impulse in a heart is usually formed in the sinoatrial node and carried through the atria, down the internodal atrial pathways to the atrioventricular node (AV) node. In normal conduction, the impulse would travel across the bundle of His, down the bundle branches, and into the Purkinje fibers. This would depolarize the ventricles and cause them to contract.

An ectopic pacemaker, also known as ectopic focus or ectopic foci, is an excitable group of cells that causes a premature heart beat outside the normally functioning SA node of the heart. It is thus a cardiac pacemaker that is ectopic, producing an ectopic beat. Acute occurrence is usually non-life-threatening, but chronic occurrence can progress into tachycardia, bradycardia or ventricular fibrillation. In a normal heart beat rhythm, the SA node usually suppresses the ectopic pacemaker activity due to the higher impulse rate of the SA node. However, in the instance of either a malfunctioning SA node or an ectopic focus bearing an intrinsic rate superior to SA node rate, ectopic pacemaker activity may take over the natural heart rhythm. This phenomenon is called an escape rhythm, the lower rhythm having escaped from the dominance of the upper rhythm. As a rule, premature ectopic beats indicate increased myocyte or conducting tissue excitability, whereas late ectopic beats indicate proximal pacemaker or conduction failure with an escape 'ectopic' beat.

Junctional ectopic tachycardia (JET) is a rare syndrome of the heart that manifests in patients recovering from heart surgery. It is characterized by cardiac arrhythmia, or irregular beating of the heart, caused by abnormal conduction from or through the atrioventricular node. In newborns and infants up to 6 weeks old, the disease may also be referred to as His bundle tachycardia or congenital JET.

Arrhythmias, also known as cardiac arrhythmias, heart arrhythmias, or dysrhythmias, are irregularities in the heartbeat, including when it is too fast or too slow. A resting heart rate that is too fast – above 100 beats per minute in adults – is called tachycardia, and a resting heart rate that is too slow – below 60 beats per minute – is called bradycardia. Some types of arrhythmias have no symptoms. Symptoms, when present, may include palpitations or feeling a pause between heartbeats. In more serious cases, there may be lightheadedness, passing out, shortness of breath, chest pain, or decreased level of consciousness. While most cases of arrhythmia are not serious, some predispose a person to complications such as stroke or heart failure. Others may result in sudden death.
An idioventricular rhythm is a cardiac rhythm characterized by a rate of <50 beats per minute (bpm), absence of P waves and widening of the QRS complex. In cases where the heart rate is between 50 and 110 bpm, it is known as accelerated idioventricular rhythm and ventricular tachycardia if the rate exceeds 120 bpm. Causes of idioventricular rhythms are varied and can include drugs or a heart defect at birth. It is typically benign and not life-threatening.