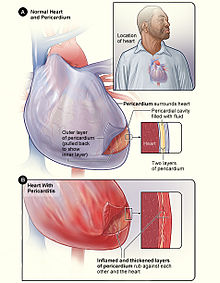
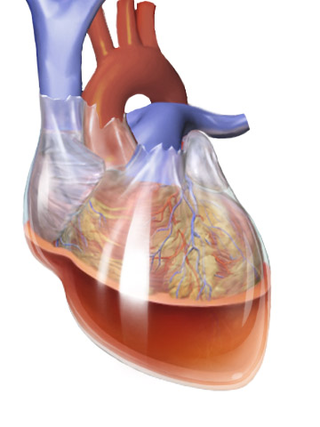
The pericardium, also called pericardial sac, is a double-walled sac containing the heart and the roots of the great vessels. It has two layers, an outer layer made of strong inelastic connective tissue, and an inner layer made of serous membrane. It encloses the pericardial cavity, which contains pericardial fluid, and defines the middle mediastinum. It separates the heart from interference of other structures, protects it against infection and blunt trauma, and lubricates the heart's movements.
Cardiac tamponade, also known as pericardial tamponade, is a compression of the heart due to pericardial effusion. Onset may be rapid or gradual. Symptoms typically include those of obstructive shock including shortness of breath, weakness, lightheadedness, and cough. Other symptoms may relate to the underlying cause.

Chest pain is pain or discomfort in the chest, typically the front of the chest. It may be described as sharp, dull, pressure, heaviness or squeezing. Associated symptoms may include pain in the shoulder, arm, upper abdomen, or jaw, along with nausea, sweating, or shortness of breath. It can be divided into heart-related and non-heart-related pain. Pain due to insufficient blood flow to the heart is also called angina pectoris. Those with diabetes or the elderly may have less clear symptoms.
Constrictive pericarditis is a condition characterized by a thickened, fibrotic pericardium, limiting the heart's ability to function normally. In many cases, the condition continues to be difficult to diagnose and therefore benefits from a good understanding of the underlying cause.

Pericardiocentesis (PCC), also called pericardial tap, is a medical procedure where fluid is aspirated from the pericardium.
Dressler syndrome is a secondary form of pericarditis that occurs in the setting of injury to the heart or the pericardium. It consists of fever, pleuritic pain, pericarditis and/or pericardial effusion.
A pericardial friction rub, also pericardial rub, is an audible medical sign used in the diagnosis of pericarditis. Upon auscultation, this sign is an extra heart sound of to-and-fro character, typically with three components, two systolic and one diastolic. It resembles the sound of squeaky leather and often is described as grating, scratching, or rasping. The sound seems very close to the ear and may seem louder than or may even mask the other heart sounds. The sound usually is best heard between the apex and sternum but may be widespread.
Pulsus paradoxus, also paradoxic pulse or paradoxical pulse, is an abnormally large decrease in stroke volume, systolic blood pressure and pulse wave amplitude during inspiration. Pulsus paradoxus is not related to pulse rate or heart rate, and it is not a paradoxical rise in systolic pressure. Normally, blood pressure drops less precipitously than 10 mmHg during inhalation. Pulsus paradoxus is a sign that is indicative of several conditions, most commonly pericardial effusion.

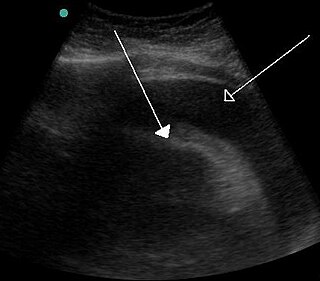
A pericardial effusion is an abnormal accumulation of fluid in the pericardial cavity. The pericardium is a two-part membrane surrounding the heart: the outer fibrous connective membrane and an inner two-layered serous membrane. The two layers of the serous membrane enclose the pericardial cavity between them. This pericardial space contains a small amount of pericardial fluid, normally 15-50 mL in volume. The pericardium, specifically the pericardial fluid provides lubrication, maintains the anatomic position of the heart in the chest, and also serves as a barrier to protect the heart from infection and inflammation in adjacent tissues and organs.

Acute pericarditis is a type of pericarditis usually lasting less than 6 weeks. It is the most common condition affecting the pericardium.
Pericardiectomy is the surgical removal of part or most of the pericardium. This operation is most commonly used to relieve constrictive pericarditis, or to remove a pericardium that is calcified and fibrous. It may also be used for severe or recurrent cases of pericardial effusion. Post-operative outcomes and mortality are significantly impacted by the disease it is used to treat.

Myocardial rupture is a laceration of the ventricles or atria of the heart, of the interatrial or interventricular septum, or of the papillary muscles. It is most commonly seen as a serious sequela of an acute myocardial infarction.
The following outline is provided as an overview of and topical guide to cardiology, the branch of medicine dealing with disorders of the human heart. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease and electrophysiology. Physicians who specialize in cardiology are called cardiologists.
Obstructive shock is one of the four types of shock, caused by a physical obstruction in the flow of blood. Obstruction can occur at the level of the great vessels or the heart itself. Causes include pulmonary embolism, cardiac tamponade, and tension pneumothorax. These are all life-threatening. Symptoms may include shortness of breath, weakness, or altered mental status. Low blood pressure and tachycardia are often seen in shock. Other symptoms depend on the underlying cause.
Hemopericardium refers to blood in the pericardial sac of the heart. It is clinically similar to a pericardial effusion, and, depending on the volume and rapidity with which it develops, may cause cardiac tamponade.
Tuberculous pericarditis is a form of pericarditis. It is a condition in which the pericardium surrounding the heart is infected by the bacterial species Mycobacterium tuberculosis. Tuberculous pericarditis accounts for a significant percentage of presentations of tuberculosis worldwide. The condition has four stages of disease which manifests with clinical presentations ranging from acute pericarditis to overt heart failure. Tuberculous pericarditis is an under-diagnosed condition. Diagnosis often requires a range of diagnostic tools, including pericardiocentesis, biochemical tests, and imaging. Treatment of this disease is similar to treatment of pulmonary tuberculosis. Alternative treatment options to reduce cardiac complications are also available.
Myocardial infarction complications may occur immediately following a myocardial infarction, or may need time to develop. After an infarction, an obvious complication is a second infarction, which may occur in the domain of another atherosclerotic coronary artery, or in the same zone if there are any live cells left in the infarct.

Postpericardiotomy syndrome (PPS) is a medical syndrome referring to an immune phenomenon that occurs days to months after surgical incision of the pericardium. PPS can also be caused after a trauma, a puncture of the cardiac or pleural structures, after percutaneous coronary intervention, or due to pacemaker or pacemaker wire placement.

Purulent pericarditis refers to localized inflammation in the setting of infection of the pericardial sac surrounding the heart. In contrast to other causes of pericarditis which may have a viral etiology, purulent pericarditis refers specifically to bacterial or fungal infection of the pericardial sac. Clinical etiologies of purulent pericarditis may include recent surgery, adjacent infection, trauma, or even primary infection. The onset of purulent pericarditis is usually acute, with most individuals presenting to a medical facility approximately 3 days following the onset of symptoms.