Related Research Articles

Fecal incontinence (FI), or in some forms encopresis, is a lack of control over defecation, leading to involuntary loss of bowel contents, both liquid stool elements and mucus, or solid feces. When this loss includes flatus (gas), it is referred to as anal incontinence. FI is a sign or a symptom, not a diagnosis. Incontinence can result from different causes and might occur with either constipation or diarrhea. Continence is maintained by several interrelated factors, including the anal sampling mechanism, and incontinence usually results from deficiency of multiple mechanisms. The most common causes are thought to be immediate or delayed damage from childbirth, complications from prior anorectal surgery, altered bowel habits, and receptive anal sex. An estimated 2.2% of community dwelling adults are affected. However, reported prevalence figures vary. A prevalence of 8.39% among non-institutionalized U.S adults between 2005 and 2010 has been reported, and among institutionalized elders figures come close to 50%.
Encopresis is voluntary or involuntary passage of feces outside of toilet-trained contexts in children who are four years or older and after an organic cause has been excluded. Children with encopresis often leak stool into their undergarments.

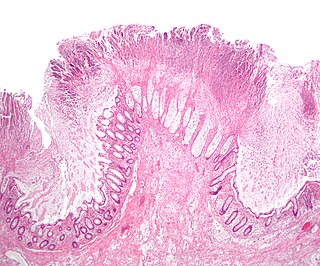
A rectal prolapse occurs when walls of the rectum have prolapsed to such a degree that they protrude out of the anus and are visible outside the body. However, most researchers agree that there are 3 to 5 different types of rectal prolapse, depending on whether the prolapsed section is visible externally, and whether the full or only partial thickness of the rectal wall is involved.

Rectal foreign bodies are large foreign items found in the rectum that can be assumed to have been inserted through the anus, rather than reaching the rectum via the mouth and gastrointestinal tract. It can be of clinical relevance if the patient cannot remove it the way they intended. Smaller, ingested foreign bodies, such as bones eaten with food, can sometimes be found stuck in the rectum upon x-ray and are rarely of clinical relevance.
Colorectal surgery is a field in medicine dealing with disorders of the rectum, anus, and colon. The field is also known as proctology, but this term is now used infrequently within medicine and is most often employed to identify practices relating to the anus and rectum in particular. The word proctology is derived from the Greek words πρωκτός proktos, meaning "anus" or "hindparts", and -λογία -logia, meaning "science" or "study".
An abdomino perineal resection, formally known as abdominoperineal resection of the rectum and abdominoperineal excision of the rectum is a surgery for rectal cancer or anal cancer. It is frequently abbreviated as AP resection, APR and APER.

Ileostomy is a stoma constructed by bringing the end or loop of small intestine out onto the surface of the skin, or the surgical procedure which creates this opening. Intestinal waste passes out of the ileostomy and is collected in an external ostomy system which is placed next to the opening. Ileostomies are usually sited above the groin on the right hand side of the abdomen.
In medicine, the ileal pouch–anal anastomosis (IPAA), also known as an ileo-anal pouch, restorative proctocolectomy, ileal-anal pullthrough, or sometimes referred to as a j-pouch, s-pouch, w-pouch or an internal pouch, is an anastomosis of the ileum to the anus, bypassing the former site of the colon in cases where the colon has been removed. It retains or restores functionality of the anus, with stools passed under voluntary control of the patient, preventing fecal incontinence and serving as an alternative to ileostomy. The pouch component is a surgically constructed intestinal reservoir; usually situated near where the rectum would normally be. It is formed by folding loops of small intestine back on themselves and stitching or stapling them together. The internal walls are then removed thus forming a reservoir. The reservoir is then stitched or stapled into the perineum where the rectum was.

A fecal impaction is a solid, immobile bulk of feces that can develop in the rectum as a result of chronic constipation. A related term is fecal loading which refers to a large volume of stool in the rectum of any consistency. Fecal impaction is a common result of neurogenic bowel dysfunction and causes immense discomfort and pain. Treatment of fecal impaction includes laxatives, enema, and pulsed irrigation evacuation (PIE). Research shows that pulsed irrigation evacuation with the PIE MED device is successful in all tested patients in studies, making pulsed irrigation evacuation the most effective and reliable form of fecal impaction treatment.
Colectomy is bowel resection of the large bowel (colon). It consists of the surgical removal of any extent of the colon, usually segmental resection. In extreme cases where the entire large intestine is removed, it is called total colectomy, and proctocolectomy denotes that the rectum is included.

Megacolon is an abnormal dilation of the colon. This leads to hypertrophy of the colon. The dilation is often accompanied by a paralysis of the peristaltic movements of the bowel. In more extreme cases, the feces consolidate into hard masses inside the colon, called fecalomas, which can require surgery to be removed.
Digestive system surgery, or gastrointestinal surgery, can be divided into upper GI surgery and lower GI surgery.
Total mesorectal excision (TME) is a standard surgical technique for treatment of rectal cancer, first described in 1982 by Professor Bill Heald at the UK's Basingstoke District Hospital. It is a precise dissection of the mesorectal envelope comprising rectum containing the tumour together with all the surrounding fatty tissue and the sheet of tissue that contains lymph nodes and blood vessels. Dissection is along the avascular alveolar plane between the presacral and mesorectal fascia, described as holy plane. Dissection along this plane facilitates a straightforward dissection and preserves the sacral vessels and hypogastric nerves and is a sphincter-sparing resection and decreases permanent stoma rates. It is possible to rejoin the two ends of the colon; however, most patients require a temporary ileostomy pouch to bypass the colon, allowing it to heal with less risk of infection, perforation or leakage.

A colorectal polyp is a polyp occurring on the lining of the colon or rectum. Untreated colorectal polyps can develop into colorectal cancer.

Defecography is a type of medical radiological imaging in which the mechanics of a patient's defecation are visualized in real time using a fluoroscope. The anatomy and function of the anorectum and pelvic floor can be dynamically studied at various stages during defecation.
A lower anterior resection, formally known as anterior resection of the rectum and colon and anterior excision of the rectum or simply anterior resection, is a common surgery for rectal cancer and occasionally is performed to remove a diseased or ruptured portion of the intestine in cases of diverticulitis. It is commonly abbreviated as LAR.

The rectum is the final straight portion of the large intestine in humans and some other mammals, and the gut in others. The adult human rectum is about 12 centimetres (4.7 in) long, and begins at the rectosigmoid junction at the level of the third sacral vertebra or the sacral promontory depending upon what definition is used. Its diameter is similar to that of the sigmoid colon at its commencement, but it is dilated near its termination, forming the rectal ampulla. It terminates at the level of the anorectal ring or the dentate line, again depending upon which definition is used. In humans, the rectum is followed by the anal canal which is about 4 centimetres (1.6 in) long, before the gastrointestinal tract terminates at the anal verge. The word rectum comes from the Latin rectumintestinum, meaning straight intestine.
Rectal discharge is intermittent or continuous expression of liquid from the anus. Normal rectal mucus is needed for proper excretion of waste. Otherwise, this is closely related to types of fecal incontinence but the term rectal discharge does not necessarily imply degrees of incontinence. Types of fecal incontinence that produce a liquid leakage could be thought of as a type of rectal discharge.
Anismus or dyssynergic defecation is the failure of normal relaxation of pelvic floor muscles during attempted defecation. It can occur in both children and adults, and in both men and women. It can be caused by physical defects or it can occur for other reasons or unknown reasons. Anismus that has a behavioral cause could be viewed as having similarities with parcopresis, or psychogenic fecal retention.
Sigmoidocele refers to a condition where the sigmoid colon descends (prolapses) into the lower pelvic cavity. This can obstruct the rectum and cause symptoms of obstructed defecation.
References
- ↑ Smith, Lee E.; Blatchford, Garnet J. (2007). "Physiologic Testing". In Wolff, Bruce G.; Fleshman, James W.; Beck, David E. (eds.). ASCRS textbook of colon and rectal surgery. New York: Springer. p. 50. ISBN 978-0-387-24846-2.