Viral meningitis, also known as aseptic meningitis, is a type of meningitis due to a viral infection. It results in inflammation of the meninges. Symptoms commonly include headache, fever, sensitivity to light and neck stiffness.

Acute septic arthritis, infectious arthritis, suppurative arthritis, pyogenic arthritis, osteomyelitis, or joint infection is the invasion of a joint by an infectious agent resulting in joint inflammation. Generally speaking, symptoms typically include redness, heat and pain in a single joint associated with a decreased ability to move the joint. Onset is usually rapid. Other symptoms may include fever, weakness and headache. Occasionally, more than one joint may be involved, especially in neonates, younger children and immunocompromised individuals. In neonates, infants during the first year of life, and toddlers, the signs and symptoms of septic arthritis can be deceptive and mimic other infectious and non-infectious disorders.

Aseptic meningitis is the inflammation of the meninges, a membrane covering the brain and spinal cord, in patients whose cerebral spinal fluid test result is negative with routine bacterial cultures. Aseptic meningitis is caused by viruses, mycobacteria, spirochetes, fungi, medications, and cancer malignancies. The testing for both meningitis and aseptic meningitis is mostly the same. A cerebrospinal fluid sample is taken by lumbar puncture and is tested for leukocyte levels to determine if there is an infection and goes on to further testing to see what the actual cause is. The symptoms are the same for both meningitis and aseptic meningitis but the severity of the symptoms and the treatment can depend on the certain cause.

Imipenem/cilastatin, sold under the brand name Primaxin among others, is an antibiotic useful for the treatment of a number of bacterial infections. It is made from a combination of imipenem and cilastatin. Specifically it is used for pneumonia, sepsis, endocarditis, joint infections, intra-abdominal infections, and urinary tract infections. It is given by injection into a vein or muscle.
Omphalitis of newborn is the medical term for inflammation of the umbilical cord stump in the neonatal newborn period, most commonly attributed to a bacterial infection. Typically immediately after an infant is born, the umbilical cord is cut with a small remnant left behind. Normally the stump separates from the skin within 3–45 days after birth. A small amount of pus-like material is commonly seen at the base of the stump and can be controlled by keeping the stump open to air to dry. Certain bacteria can grow and infect the stump during this process and as a result significant redness and swelling may develop, and in some cases the infection can then spread through the umbilical vessels to the rest of the body. While currently an uncommon anatomical location for infection in the newborn in the United States, it has caused significant morbidity and mortality both historically and in areas where health care is less readily available. In general, when this type of infection is suspected or diagnosed, antibiotic treatment is given, and in cases of serious complications surgical management may be appropriate.

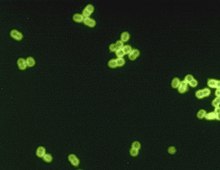
Streptococcus agalactiae is a gram-positive coccus with a tendency to form chains. It is a beta-hemolytic, catalase-negative, and facultative anaerobe.
Community-acquired pneumonia (CAP) refers to pneumonia contracted by a person outside of the healthcare system. In contrast, hospital-acquired pneumonia (HAP) is seen in patients who have recently visited a hospital or who live in long-term care facilities. CAP is common, affecting people of all ages, and its symptoms occur as a result of oxygen-absorbing areas of the lung (alveoli) filling with fluid. This inhibits lung function, causing dyspnea, fever, chest pains and cough.
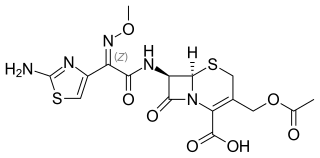
Cefotaxime is an antibiotic used to treat a number of bacterial infections in human, other animals and plant tissue culture. Specifically in humans it is used to treat joint infections, pelvic inflammatory disease, meningitis, pneumonia, urinary tract infections, sepsis, gonorrhea, and cellulitis. It is given either by injection into a vein or muscle.

Amikacin is an antibiotic medication used for a number of bacterial infections. This includes joint infections, intra-abdominal infections, meningitis, pneumonia, sepsis, and urinary tract infections. It is also used for the treatment of multidrug-resistant tuberculosis. It is used by injection into a vein using an IV or into a muscle.
Group B streptococcal infection, also known as Group B streptococcal disease or just Group B strep infection, is the infectious disease caused by the bacterium Streptococcus agalactiae, which is the most common human pathogen belonging to the group B of the Lancefield classification of streptococci—hence the group B stretococcal (GBS) infection nomenclature. Infection with GBS can cause serious illness and sometimes death, especially in newborns, the elderly, and people with compromised immune systems. The most severe form of group B streptococcal disease is neonatal meningitis in infants, which is frequently lethal and can cause permanent neuro-cognitive impairment.

Chorioamnionitis, also known as intra-amniotic infection (IAI), is inflammation of the fetal membranes, usually due to bacterial infection. In 2015, a National Institute of Child Health and Human Development Workshop expert panel recommended use of the term "triple I" to address the heterogeneity of this disorder. The term triple I refers to intrauterine infection or inflammation or both and is defined by strict diagnostic criteria, but this terminology has not been commonly adopted although the criteria are used.

Neonatal conjunctivitis is a form of conjunctivitis which affects newborn babies following birth. It is typically due to neonatal bacterial infection, although it can also be non-infectious. Infectious neonatal conjunctivitis is typically contracted during vaginal delivery from exposure to bacteria from the birth canal, most commonly Neisseria gonorrhoeae or Chlamydia trachomatis.

Cefquinome is a fourth-generation cephalosporin with pharmacological and antibacterial properties valuable in the treatment of coliform mastitis and other infections. It is only used in veterinary applications.

Corneal ulcer, also called keratitis, is an inflammatory or, more seriously, infective condition of the cornea involving disruption of its epithelial layer with involvement of the corneal stroma. It is a common condition in humans particularly in the tropics and in farming. In developing countries, children afflicted by vitamin A deficiency are at high risk for corneal ulcer and may become blind in both eyes persisting throughout life. In ophthalmology, a corneal ulcer usually refers to having an infection, while the term corneal abrasion refers more to a scratch injury.
Mollaret's meningitis is a recurrent or chronic inflammation of the protective membranes covering the brain and spinal cord, known collectively as the meninges. Since Mollaret's meningitis is a recurrent, benign (non-cancerous), aseptic meningitis, it is also referred to as benign recurrent lymphocytic meningitis. It was named for Pierre Mollaret, the French neurologist who first described it in 1944.
Meningitis is acute or chronic inflammation of the protective membranes covering the brain and spinal cord, collectively called the meninges. The most common symptoms are fever, intense headache, vomiting and neck stiffness and occasionally photophobia.
Neonatal herpes simplex, or simply neonatal herpes, is a herpes infection in a newborn baby caused by the herpes simplex virus (HSV), mostly as a result of vertical transmission of the HSV from an affected mother to her baby. Types include skin, eye, and mouth herpes (SEM), disseminated herpes (DIS), and central nervous system herpes (CNS). Depending on the type, symptoms vary from a fever to small blisters, irritability, low body temperature, lethargy, breathing difficulty, and a large abdomen due to ascites or large liver. There may be red streaming eyes or no symptoms.
Neonatal sepsis is a type of neonatal infection and specifically refers to the presence in a newborn baby of a bacterial blood stream infection (BSI) in the setting of fever. Older textbooks may refer to neonatal sepsis as "sepsis neonatorum". Criteria with regards to hemodynamic compromise or respiratory failure are not useful clinically because these symptoms often do not arise in neonates until death is imminent and unpreventable. Neonatal sepsis is divided into two categories: early-onset sepsis (EOS) and late-onset sepsis (LOS). EOS refers to sepsis presenting in the first 7 days of life, with LOS referring to presentation of sepsis after 7 days. Neonatal sepsis is the single most common cause of neonatal death in hospital as well as community in developing country.
Citrobacter koseri, formerly known as Citrobacter diversus, is a Gram-negative non-spore forming, rod-shaped bacterium. It is a facultative anaerobe capable of aerobic respiration. It is motile via peritrichous flagella. It is a member of the family of Enterobacteriaceae. The members of this family are part of the normal flora and commonly found in the digestive tracts of humans and animals. C. koseri may act as an opportunistic pathogen in individuals who are immunocompromised.

Neonatal infections are infections of the neonate (newborn) acquired during prenatal development or within the first four weeks of life. Neonatal infections may be contracted by mother to child transmission, in the birth canal during childbirth, or after birth. Neonatal infections may present soon after delivery, or take several weeks to show symptoms. Some neonatal infections such as HIV, hepatitis B, and malaria do not become apparent until much later. Signs and symptoms of infection may include respiratory distress, temperature instability, irritability, poor feeding, failure to thrive, persistent crying and skin rashes.