
Positron emission tomography (PET) is a functional imaging technique that uses radioactive substances known as radiotracers to visualize and measure changes in metabolic processes, and in other physiological activities including blood flow, regional chemical composition, and absorption. Different tracers are used for various imaging purposes, depending on the target process within the body.

Radiology is the medical specialty that uses medical imaging to diagnose diseases and guide their treatment, within the bodies of humans and other animals. It began with radiography, but today it includes all imaging modalities, including those that use no ionizing electromagnetic radiation, as well as others that do, such as computed tomography (CT), fluoroscopy, and nuclear medicine including positron emission tomography (PET). Interventional radiology is the performance of usually minimally invasive medical procedures with the guidance of imaging technologies such as those mentioned above.
Pheochromocytoma is a rare tumor of the adrenal medulla composed of chromaffin cells, also known as pheochromocytes. When a tumor composed of the same cells as a pheochromocytoma develops outside the adrenal gland, it is referred to as a paraganglioma. These neuroendocrine tumors typically release massive amounts of catecholamines which result in the most common symptoms, including hypertension, tachycardia, and sweating. Rarely, some tumors may secrete little to no catecholamines, making diagnosis difficult. While tumors of the head and neck are parasympathetic, their sympathetic counterparts are predominantly located in the abdomen and pelvis, particularly concentrated at the organ of Zuckerkandl.

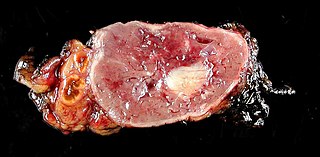
Hemangiosarcoma is a rapidly growing, highly invasive variety of cancer that occurs almost exclusively in dogs, and only rarely in cats, horses, mice, or humans. It is a sarcoma arising from the lining of blood vessels; that is, blood-filled channels and spaces are commonly observed microscopically. A frequent cause of death is the rupturing of this tumor, causing the patient to rapidly bleed to death.

Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal neoplasms of the gastrointestinal tract. GISTs arise in the smooth muscle pacemaker interstitial cell of Cajal, or similar cells. They are defined as tumors whose behavior is driven by mutations in the KIT gene (85%), PDGFRA gene (10%), or BRAF kinase (rare). 95% of GISTs stain positively for KIT (CD117). Most (66%) occur in the stomach and gastric GISTs have a lower malignant potential than tumors found elsewhere in the GI tract.
In medical or research imaging, an incidental imaging finding is an unanticipated finding which is not related to the original diagnostic inquiry. As with other types of incidental medical findings, they may represent a diagnostic, ethical, and philosophical dilemma because their significance is unclear. While some coincidental findings may lead to beneficial diagnoses, others may lead to overdiagnosis that results in unnecessary testing and treatment, sometimes called the "cascade effect".

Neuroendocrine tumors (NETs) are neoplasms that arise from cells of the endocrine (hormonal) and nervous systems. They most commonly occur in the intestine, where they are often called carcinoid tumors, but they are also found in the pancreas, lung, and the rest of the body.
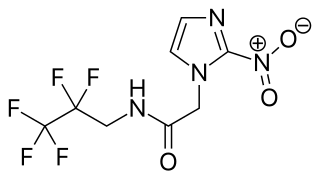
EF5 is a nitroimidazole derivative used in oncology research. Due to its similarity in chemical structure to etanidazole, EF5 binds in cells displaying hypoxia.

A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.

Bone metastasis, or osseous metastatic disease, is a category of cancer metastases that result from primary tumor invasions into bones. Bone-originating primary tumors such as osteosarcoma, chondrosarcoma, and Ewing sarcoma are rare; the most common bone tumor is a metastasis. Bone metastases can be classified as osteolytic, osteoblastic, or both. Unlike hematologic malignancies which originate in the blood and form non-solid tumors, bone metastases generally arise from epithelial tumors and form a solid mass inside the bone. Bone metastases, especially in a state of advanced disease, can cause severe pain, characterized by a dull, constant ache with periodic spikes of incident pain.

Positron emission tomography–magnetic resonance imaging (PET–MRI) is a hybrid imaging technology that incorporates magnetic resonance imaging (MRI) soft tissue morphological imaging and positron emission tomography (PET) functional imaging.

Positron emission mammography (PEM) is a nuclear medicine imaging modality used to detect or characterise breast cancer. Mammography typically refers to x-ray imaging of the breast, while PEM uses an injected positron emitting isotope and a dedicated scanner to locate breast tumors. Scintimammography is another nuclear medicine breast imaging technique, however it is performed using a gamma camera. Breasts can be imaged on standard whole-body PET scanners, however dedicated PEM scanners offer advantages including improved resolution.

18F-FMISO or fluoromisonidazole is a radiopharmaceutical used for PET imaging of hypoxia. It consists of a 2-nitroimidazole molecule labelled with the positron-emitter fluorine-18.
PI-RADS is an acronym for Prostate Imaging Reporting and Data System, defining standards of high-quality clinical service for multi-parametric magnetic resonance imaging (mpMRI), including image creation and reporting.
CAPP-Seq is a next-generation sequencing based method used to quantify circulating DNA in cancer (ctDNA). The method was introduced in 2014 by Ash Alizadeh and Maximilian Diehn’s laboratories at Stanford, as a tool for measuring Cell-free tumor DNA which is released from dead tumor cells into the blood and thus may reflect the entire tumor genome. This method can be generalized for any cancer type that is known to have recurrent mutations. CAPP-Seq can detect one molecule of mutant DNA in 10,000 molecules of healthy DNA. The original method was further refined in 2016 for ultra sensitive detection through integration of multiple error suppression strategies, termed integrated Digital Error Suppression (iDES). The use of ctDNA in this technique should not be confused with circulating tumor cells (CTCs); these are two different entities.

Fluciclovine (18F), also known as anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid, or as Axumin, is a diagnostic agent indicated for positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated prostate specific antigen (PSA) levels.

Andreas Kjær is a Danish physician-scientist and European Research Council (ERC) advanced grantee. He is professor at the University of Copenhagen and chief physician at Rigshospitalet, the National University Hospital of Denmark. He is board certified in Nuclear Medicine and his research is focused on molecular imaging with PET and PET/MRI and targeted radionuclide therapies (theranostics) in cancer. His achievements include development of several new PET tracers that have reached first-in-human clinical use. He has published more than 400 peer-review articles, filed 10 patents, supervised more than 40 PhD students and received numerous prestigious scientific awards over the years. He is a member of the Danish Academy of Technical Sciences
Jason S. Lewis is a British radiochemist whose work relates to oncologic therapy and diagnosis. His research focus is a molecular imaging-based program focused on radiopharmaceutical development as well as the study of multimodality small- and biomolecule-based agents and their clinical translation. He has worked on the development of small molecules as well as radiolabeled peptides and antibodies probing the overexpression of receptors and antigens on tumors.

Papillary renal cell carcinoma (PRCC) is a malignant, heterogeneous tumor originating from renal tubular epithelial cells of the kidney, which comprises approximately 10-15% of all kidney neoplasms. Based on its morphological features, PRCC can be classified into two main subtypes, which are type 1 (basophilic) and type 2 (eosinophilic).
Vicky Goh is a professor, chair of clinical cancer imaging, and head of cancer imaging department at the King's College London, England, United Kingdom. She joined King's College London in 2011. She is also a consultant radiologist at Guy's and St Thomas' Hospital in London.