
An arteriovenous malformation (AVM) is an abnormal connection between arteries and veins, bypassing the capillary system. Usually congenital, this vascular anomaly is widely known because of its occurrence in the central nervous system, but can appear anywhere in the body. The symptoms of AVMs can range from none at all to intense pain or bleeding, and they can lead to other serious medical problems.

A cerebral arteriovenous malformation is an abnormal connection between the arteries and veins in the brain—specifically, an arteriovenous malformation in the cerebrum.

Cerebrovascular disease includes a variety of medical conditions that affect the blood vessels of the brain and the cerebral circulation. Arteries supplying oxygen and nutrients to the brain are often damaged or deformed in these disorders. The most common presentation of cerebrovascular disease is an ischemic stroke or mini-stroke and sometimes a hemorrhagic stroke. Hypertension is the most important contributing risk factor for stroke and cerebrovascular diseases as it can change the structure of blood vessels and result in atherosclerosis. Atherosclerosis narrows blood vessels in the brain, resulting in decreased cerebral perfusion. Other risk factors that contribute to stroke include smoking and diabetes. Narrowed cerebral arteries can lead to ischemic stroke, but continually elevated blood pressure can also cause tearing of vessels, leading to a hemorrhagic stroke.
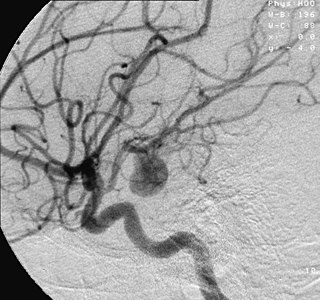
An aneurysm is an outward bulging, likened to a bubble or balloon, caused by a localized, abnormal, weak spot on a blood vessel wall. Aneurysms may be a result of a hereditary condition or an acquired disease. Aneurysms can also be a nidus for clot formation (thrombosis) and embolization. As an aneurysm increases in size, the risk of rupture, which leads to uncontrolled bleeding, increases. Although they may occur in any blood vessel, particularly lethal examples include aneurysms of the circle of Willis in the brain, aortic aneurysms affecting the thoracic aorta, and abdominal aortic aneurysms. Aneurysms can arise in the heart itself following a heart attack, including both ventricular and atrial septal aneurysms. There are congenital atrial septal aneurysms, a rare heart defect.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

Subarachnoid hemorrhage (SAH) is bleeding into the subarachnoid space—the area between the arachnoid membrane and the pia mater surrounding the brain. Symptoms may include a severe headache of rapid onset, vomiting, decreased level of consciousness, fever, weakness, numbness, and sometimes seizures. Neck stiffness or neck pain are also relatively common. In about a quarter of people a small bleed with resolving symptoms occurs within a month of a larger bleed.

Intracranial hemorrhage (ICH), also known as intracranial bleed, is bleeding within the skull. Subtypes are intracerebral bleeds, subarachnoid bleeds, epidural bleeds, and subdural bleeds.

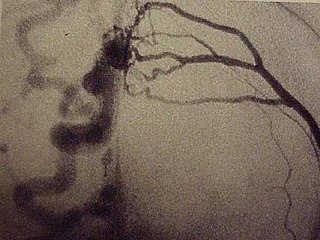
Cerebral angiography is a form of angiography which provides images of blood vessels in and around the brain, thereby allowing detection of abnormalities such as arteriovenous malformations and aneurysms. It was pioneered in 1927 by the Portuguese neurologist Egas Moniz at the University of Lisbon, who also helped develop thorotrast for use in the procedure.
A thunderclap headache is a headache that is severe and has a sudden onset. It is defined as a severe headache that takes seconds to minutes to reach maximum intensity. Although approximately 75% are attributed to "primary" headaches—headache disorder, non-specific headache, idiopathic thunderclap headache, or uncertain headache disorder—the remainder are secondary to other causes, which can include some extremely dangerous acute conditions, as well as infections and other conditions. Usually, further investigations are performed to identify the underlying cause.
The International Subarachnoid Aneurysm Trial (ISAT) was a large multicentre, prospective randomised clinical medical trial, comparing the safety and efficacy of endovascular coil treatment and surgical clipping for the treatment of brain aneurysms. The study began in 1994. The first results were published in The Lancet in 2002, and the 10 year data were published again in The Lancet in early September 2005. 2,143 study participants were mostly drawn from U.K. hospitals with the rest drawn from North American and European hospitals.
Intracerebral hemorrhage (ICH), also known as hemorrhagic stroke, is a sudden bleeding into the tissues of the brain, into its ventricles, or into both. An ICH is a type of bleeding within the skull and one kind of stroke. Symptoms can vary dramatically depending on the severity, acuity, and location (anatomically) but can include headache, one-sided weakness, numbness, tingling, or paralysis, speech problems, vision or hearing problems, memory loss, attention problems, coordination problems, balance problems, dizziness or lightheadedness or vertigo, nausea/vomiting, seizures, decreased level of consciousness or total loss of consciousness, neck stiffness, and fever.
A dural arteriovenous fistula (DAVF) or malformation is an abnormal direct connection (fistula) between a meningeal artery and a meningeal vein or dural venous sinus.

Vertebral artery dissection (VAD) is a flap-like tear of the inner lining of the vertebral artery, which is located in the neck and supplies blood to the brain. After the tear, blood enters the arterial wall and forms a blood clot, thickening the artery wall and often impeding blood flow. The symptoms of vertebral artery dissection include head and neck pain and intermittent or permanent stroke symptoms such as difficulty speaking, impaired coordination, and visual loss. It is usually diagnosed with a contrast-enhanced CT or MRI scan.
The Center for Cerebrovascular Research at the University of California, San Francisco is a collective of faculty and staff investigating matters related to cerebral circulation, particularly cerebrovascular disease resulting from narrowing of major blood vessels in the brain and vascular malformation of the brain. While research offices are located on Parnassus campus, San Francisco General Hospital hosts the center's laboratories and facilities. The center coordinates with additional faculty in various fields of neuroscience and vascular biology. Sponsors include the National Institute of Neurological Disorders and Stroke and the UCSF departments of Anesthesia, Neurological Surgery and Neurology.
Joshua B. Bederson is an American neurosurgeon, Leonard I. Malis, MD/Corinne and Joseph Graber Professor of Neurosurgery, and System Chair of Neurosurgery at the Mount Sinai Health System in New York City. He is a Fellow of the American College of Surgeons, and an attending neurosurgeon at The Mount Sinai Hospital.

Endovascular coiling is an endovascular treatment for intracranial aneurysms and bleeding throughout the body. The procedure reduces blood circulation to the aneurysm through the use of microsurgical detachable platinum wires, with the clinician inserting one or more into the aneurysm until it is determined that blood flow is no longer occurring within the space. It is one of two main treatments for cerebral aneurysms, the other being surgical clipping. Clipping is an alternative to stenting for bleeding.
Interventional neuroradiology (INR) also known as neurointerventional surgery (NIS), endovascular therapy (EVT), endovascular neurosurgery, and interventional neurology is a medical subspecialty of neurosurgery, neuroradiology, intervention radiology and neurology specializing in minimally invasive image-based technologies and procedures used in diagnosis and treatment of diseases of the head, neck, and spine.
An infectious intracranial aneurysm is a cerebral aneurysm that is caused by infection of the cerebral arterial wall.
Alexander Coon is an American neurosurgeon who is the Director of Endovascular and Cerebrovascular Neurosurgery at the Carondelet Neurological Institute of St. Joseph's and St. Mary's Hospitals in Tucson, Arizona. He was previously the Director of Endovascular Neurosurgery at the Johns Hopkins Hospital and an assistant professor of neurosurgery, Neurology, and Radiology at the Johns Hopkins Hospital. He is known for his work in cerebrovascular and endovascular neurosurgery and his research in neuroendovascular devices and clinical outcomes in the treatment of cerebral aneurysms, subarachnoid hemorrhage, and AVMs.

Clazosentan is a drug belonging to the class of endothelin receptor antagonists.




