
Giant cell arteritis (GCA), also called temporal arteritis, is an inflammatory autoimmune disease of large blood vessels. Symptoms may include headache, pain over the temples, flu-like symptoms, double vision, and difficulty opening the mouth. Complication can include blockage of the artery to the eye with resulting blindness, as well as aortic dissection, and aortic aneurysm. GCA is frequently associated with polymyalgia rheumatica.

Aortic dissection (AD) occurs when an injury to the innermost layer of the aorta allows blood to flow between the layers of the aortic wall, forcing the layers apart. In most cases, this is associated with a sudden onset of severe chest or back pain, often described as "tearing" in character. Vomiting, sweating, and lightheadedness may also occur. Damage to other organs may result from the decreased blood supply, such as stroke, lower extremity ischemia, or mesenteric ischemia. Aortic dissection can quickly lead to death from insufficient blood flow to the heart or complete rupture of the aorta.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

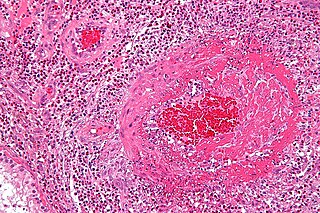
Vasculitis is a group of disorders that destroy blood vessels by inflammation. Both arteries and veins are affected. Lymphangitis is sometimes considered a type of vasculitis. Vasculitis is primarily caused by leukocyte migration and resultant damage. Although both occur in vasculitis, inflammation of veins (phlebitis) or arteries (arteritis) on their own are separate entities.

Granulomatosis with polyangiitis (GPA), also known as Wegener's granulomatosis (WG), after the German physician Friedrich Wegener, is a rare long-term systemic disorder that involves the formation of granulomas and inflammation of blood vessels (vasculitis). It is an autoimmune disease and a form of vasculitis that affects small- and medium-size vessels in many organs but most commonly affects the upper respiratory tract, lungs and kidneys. The signs and symptoms of GPA are highly varied and reflect which organs are supplied by the affected blood vessels. Typical signs and symptoms include nosebleeds, stuffy nose and crustiness of nasal secretions, and inflammation of the uveal layer of the eye. Damage to the heart, lungs and kidneys can be fatal.
Eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as allergic granulomatosis, is an extremely rare autoimmune condition that causes inflammation of small and medium-sized blood vessels (vasculitis) in persons with a history of airway allergic hypersensitivity (atopy).

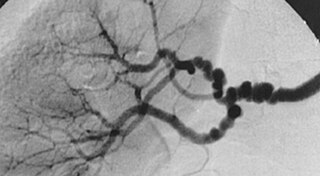
Polyarteritis nodosa (PAN) is a systemic necrotizing inflammation of blood vessels (vasculitis) affecting medium-sized muscular arteries, typically involving the arteries of the kidneys and other internal organs but generally sparing the lungs' circulation. Small aneurysms are strung like the beads of a rosary, therefore making this "rosary sign" an important diagnostic feature of the vasculitis. PAN is sometimes associated with infection by the hepatitis B or hepatitis C virus. The condition may be present in infants.

In medicine, aortoiliac occlusive disease is a form of central artery disease involving the blockage of the abdominal aorta as it transitions into the common iliac arteries.

Takayasu's arteritis (TA), also known as aortic arch syndrome, nonspecific aortoarteritis, and pulseless disease, is a form of large vessel granulomatous vasculitis with massive intimal fibrosis and vascular narrowing, most commonly affecting young or middle-aged women of Asian descent, though anyone can be affected. It mainly affects the aorta and its branches, as well as the pulmonary arteries. Females are about 8–9 times more likely to be affected than males.

Polymyalgia rheumatica (PMR) is a syndrome experienced as pain or stiffness, usually in the neck, shoulders, upper arms, and hips, but which may occur all over the body. The pain can be sudden or can occur gradually over a period. Most people with PMR wake up in the morning with pain in their muscles; however, cases have occurred in which the person has developed the pain during the evenings or has pain and stiffness all day long.
Posterior ischemic optic neuropathy (PION) is a medical condition characterized by damage to the retrobulbar portion of the optic nerve due to inadequate blood flow (ischemia) to the optic nerve. Despite the term posterior, this form of damage to the eye's optic nerve due to poor blood flow also includes cases where the cause of inadequate blood flow to the nerve is anterior, as the condition describes a particular mechanism of visual loss as much as the location of damage in the optic nerve. In contrast, anterior ischemic optic neuropathy (AION) is distinguished from PION by the fact that AION occurs spontaneously and on one side in affected individuals with predisposing anatomic or cardiovascular risk factors.
Fibromuscular dysplasia (FMD) is a non-atherosclerotic, non-inflammatory disease of the blood vessels that causes abnormal growth within the wall of an artery. FMD has been found in nearly every arterial bed in the body, although the most commonly affected are the renal and carotid arteries.

Subclavian steal syndrome (SSS), also called subclavian steal steno-occlusive disease, is a constellation of signs and symptoms that arise from retrograde (reversed) blood flow in the vertebral artery or the internal thoracic artery, due to a proximal stenosis (narrowing) and/or occlusion of the subclavian artery. This flow reversal is called the subclavian steal or subclavian steal phenomenon, regardless of signs/symptoms being present. The arm may be supplied by blood flowing in a retrograde direction down the vertebral artery at the expense of the vertebrobasilar circulation. It is more severe than typical vertebrobasilar insufficiency.
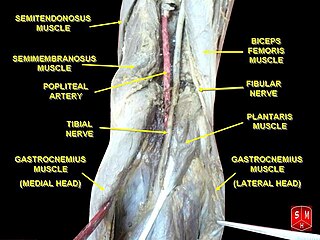
The popliteal artery entrapment syndrome (PAES) is an uncommon pathology that occurs when the popliteal artery is compressed by the surrounding popliteal fossa myofascial structures. This results in claudication and chronic leg ischemia. This condition mainly occurs more in young athletes than in the elderlies. Elderlies, who present with similar symptoms, are more likely to be diagnosed with peripheral artery disease with associated atherosclerosis. Patients with PAES mainly present with intermittent feet and calf pain associated with exercises and relieved with rest. PAES can be diagnosed with a combination of medical history, physical examination, and advanced imaging modalities such as duplex ultrasound, computer tomography, or magnetic resonance angiography. Management can range from non-intervention to open surgical decompression with a generally good prognosis. Complications of untreated PAES can include stenotic artery degeneration, complete popliteal artery occlusion, distal arterial thromboembolism, or even formation of an aneurysm.

Computed tomography angiography is a computed tomography technique used for angiography—the visualization of arteries and veins—throughout the human body. Using contrast injected into the blood vessels, images are created to look for blockages, aneurysms, dissections, and stenosis. CTA can be used to visualize the vessels of the heart, the aorta and other large blood vessels, the lungs, the kidneys, the head and neck, and the arms and legs. CTA can also be used to localise arterial or venous bleed of the gastrointestinal system.
Aortitis is the inflammation of the aortic wall. The disorder is potentially life-threatening and rare. It is reported that there are only 1–3 new cases of aortitis per year per million people in the United States and Europe. Aortitis is most common in people 10 to 40 years of age.
The following outline is provided as an overview of and topical guide to cardiology, the branch of medicine dealing with disorders of the human heart. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease and electrophysiology. Physicians who specialize in cardiology are called cardiologists.
Cerebral vasculitis is vasculitis involving the brain and occasionally the spinal cord. It affects all of the vessels: very small blood vessels (capillaries), medium-size blood vessels, or large blood vessels. If blood flow in a vessel with vasculitis is reduced or stopped, the parts of the body that receive blood from that vessel begins to die. It may produce a wide range of neurological symptoms, such as headache, skin rashes, feeling very tired, joint pains, difficulty moving or coordinating part of the body, changes in sensation, and alterations in perception, thought or behavior, as well as the phenomena of a mass lesion in the brain leading to coma and herniation. Some of its signs and symptoms may resemble multiple sclerosis. 10% have associated bleeding in the brain.

Necrotizing vasculitis, also called systemic necrotizing vasculitis, is a general term for the inflammation of veins and arteries that develops into necrosis and narrows the vessels.

Coronary CT angiography is the use of computed tomography (CT) angiography to assess the coronary arteries of the heart. The patient receives an intravenous injection of radiocontrast and then the heart is scanned using a high speed CT scanner, allowing physicians to assess the extent of occlusion in the coronary arteries, usually in order to diagnose coronary artery disease.
