| Alcoholism | |
|---|---|
| Other names | Alcohol addiction, alcohol dependence syndrome, alcohol use disorder (AUD) [1] |
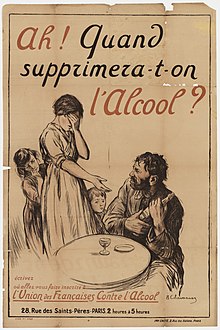 | |
| A French temperance organisation poster depicting the effects of alcoholism in a family, c. 1915: "Ah! When will we be rid of alcohol?" | |
| Specialty | Psychiatry, clinical psychology, toxicology, addiction medicine |
| Symptoms | Drinking large amounts of alcohol over a long period, difficulty cutting down, acquiring and drinking alcohol taking up a lot of time, usage resulting in problems, withdrawal occurring when stopping [2] |
| Complications | Mental illness, delirium, Wernicke–Korsakoff syndrome, irregular heartbeat, cirrhosis of the liver, cancer, fetal alcohol spectrum disorder, suicide [3] [4] [5] [6] |
| Duration | Long term [2] |
| Causes | Environmental and genetic factors [4] |
| Risk factors | Stress, anxiety, easy access [4] [7] |
| Diagnostic method | Questionnaires, blood tests [4] |
| Treatment | Alcohol cessation typically with benzodiazepines, counselling, acamprosate, disulfiram, naltrexone [8] [9] [10] Alcoholics Anonymous (AA) and other Twelve Step Programs, AA/Twelve Step Facilitation (AA/TSF) [11] |
| Frequency | 380 million / 5.1% adults (2016) [12] [13] |
| Deaths | 3.3 million / 5.9% [14] |
Alcoholism is the continued drinking of alcohol despite it causing problems. Some definitions require evidence of dependence and withdrawal. [15] Problematic use of alcohol has been mentioned in the earliest historical records. The World Health Organization (WHO) estimated there were 283 million people with alcohol use disorders worldwide as of 2016 [update] . [12] [13] The term alcoholism was first coined in 1852, [16] but alcoholism and alcoholic are stigmatizing and discourage seeking treatment, so clinical diagnostic terms such as alcohol use disorder or alcohol dependence are used instead. [17] [18]
Contents
- Signs and symptoms
- Long-term misuse
- Warning signs
- Alcohol withdrawal
- Causes
- Availability
- Gender difference
- Genetic variation
- DNA damage
- Diagnosis
- Definition
- Social barriers
- Screening
- Urine and blood tests
- Prevention
- Management
- Cessation of alcohol intake
- Psychological
- Moderate drinking
- Medications
- Research
- Dual addictions and dependencies
- Epidemiology
- Prognosis
- History
- Society and culture
- See also
- Notes
- References
- External links
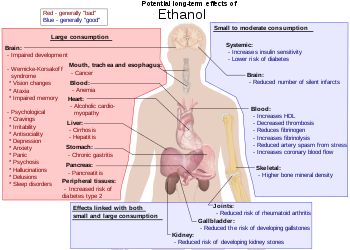
Alcohol is addictive, and heavy long-term alcohol use results in many negative health and social consequences. It can damage all the organ systems, but especially affects the brain, heart, liver, pancreas and immune system. [4] [5] Heavy alcohol usage can result in trouble sleeping, and severe cognitive issues like dementia, brain damage, or Wernicke–Korsakoff syndrome. Physical effects include irregular heartbeat, an impaired immune response, liver cirrhosis, increased cancer risk, and severe withdrawal symptoms if stopped suddenly. [4] [5] [19] These health effects can reduce life expectancy by 10 years. [20] Drinking during pregnancy may harm the child's health, [3] and drunk driving increases the risk of traffic accidents. Alcoholism is also associated with increases in violent and non-violent crime. [21] While alcoholism directly resulted in 139,000 deaths worldwide in 2013, [22] in 2012 3.3 million deaths may be attributable globally to alcohol. [14]
The development of alcoholism is attributed to both environment and genetics equally. [4] The use of alcohol to self-medicate stress or anxiety can turn into alcoholism. [23] Someone with a parent or sibling with an alcohol use disorder is three to four times more likely to develop an alcohol use disorder themselves, but only a minority of them do. [4] Environmental factors include social, cultural and behavioral influences. [24] High stress levels and anxiety, as well as alcohol's inexpensive cost and easy accessibility, increase the risk. [4] [7] People may continue to drink partly to prevent or improve symptoms of withdrawal. [4] After a person stops drinking alcohol, they may experience a low level of withdrawal lasting for months. [4] Medically, alcoholism is considered both a physical and mental illness. [25] [26] Questionnaires are usually used to detect possible alcoholism. [4] [27] Further information is then collected to confirm the diagnosis. [4]
Treatment of alcoholism may take several forms. [9] Due to medical problems that can occur during withdrawal, alcohol cessation should be controlled carefully. [9] One common method involves the use of benzodiazepine medications, such as diazepam. [9] These can be taken while admitted to a health care institution or individually. [9] The medications acamprosate or disulfiram may also be used to help prevent further drinking. [10] Mental illness or other addictions may complicate treatment. [28] Various individual or group therapy or support groups are used to attempt to keep a person from returning to alcoholism. [8] [29] Among them is the abstinence based mutual aid fellowship Alcoholics Anonymous (AA). A 2020 scientific review found that clinical interventions encouraging increased participation in AA (AA/twelve step facilitation (AA/TSF))—resulted in higher abstinence rates over other clinical interventions, and most studies in the review found that AA/TSF led to lower health costs. [lower-alpha 1] [31] [32] [33]
Many terms, some slurs and some informal, have been used to refer to people affected by alcoholism such as tippler, drunkard, dipsomaniac and souse. [34]