
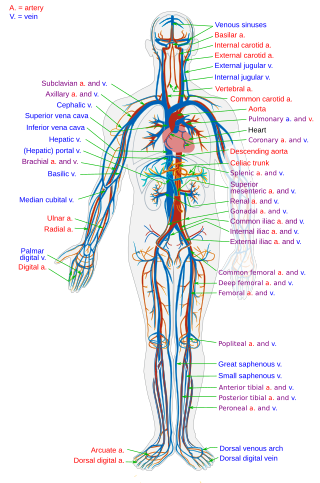
Veins are blood vessels in the circulatory system of humans and most other animals that carry blood towards the heart. Most veins carry deoxygenated blood from the tissues back to the heart; exceptions are those of the pulmonary and fetal circulations which carry oxygenated blood to the heart. In the systemic circulation, arteries carry oxygenated blood away from the heart, and veins return deoxygenated blood to the heart, in the deep veins.
The circulatory system is a system of organs that includes the heart, blood vessels, and blood which is circulated throughout the entire body of a human or other vertebrate. It includes the cardiovascular system, or vascular system, that consists of the heart and blood vessels. The circulatory system has two divisions, a systemic circulation or circuit, and a pulmonary circulation or circuit. Some sources use the terms cardiovascular system and vascular system interchangeably with circulatory system.

The superior vena cava (SVC) is the superior of the two venae cavae, the great venous trunks that return deoxygenated blood from the systemic circulation to the right atrium of the heart. It is a large-diameter (24 mm) short length vein that receives venous return from the upper half of the body, above the diaphragm. Venous return from the lower half, below the diaphragm, flows through the inferior vena cava. The SVC is located in the anterior right superior mediastinum. It is the typical site of central venous access via a central venous catheter or a peripherally inserted central catheter. Mentions of "the cava" without further specification usually refer to the SVC.

The inferior vena cava is a large vein that carries the deoxygenated blood from the lower and middle body into the right atrium of the heart. It is formed by the joining of the right and the left common iliac veins, usually at the level of the fifth lumbar vertebra.
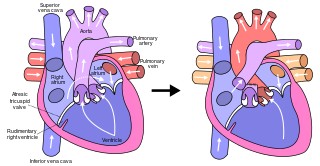
The pulmonary veins are the veins that transfer oxygenated blood from the lungs to the heart. The largest pulmonary veins are the four main pulmonary veins, two from each lung that drain into the left atrium of the heart. The pulmonary veins are part of the pulmonary circulation.

Atrial septal defect (ASD) is a congenital heart defect in which blood flows between the atria of the heart. Some flow is a normal condition both pre-birth and immediately post-birth via the foramen ovale; however, when this does not naturally close after birth it is referred to as a patent (open) foramen ovale (PFO). It is common in patients with a congenital atrial septal aneurysm (ASA).
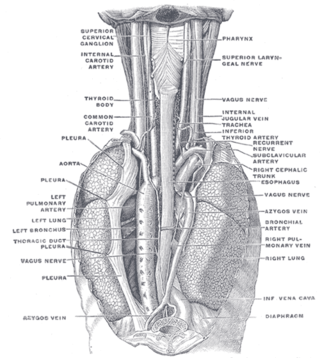
The azygos vein is a vein running up the right side of the thoracic vertebral column draining itself towards the superior vena cava. It connects the systems of superior vena cava and inferior vena cava and can provide an alternative path for blood to the right atrium when either of the venae cavae is blocked.
The Fontan procedure or Fontan–Kreutzer procedure is a palliative surgical procedure used in children with univentricular hearts. It involves diverting the venous blood from the inferior vena cava (IVC) and superior vena cava (SVC) to the pulmonary arteries. The procedure varies for differing congenital heart pathologies. For example in tricuspid atresia, the procedure can be done where the blood does not pass through the morphologic right ventricle; i.e., the systemic and pulmonary circulations are placed in series with the functional single ventricle. Whereas in hypoplastic left heart syndrome, the heart is more reliant on the more functional right ventricle to provide blood flow to the systemic circulation. The procedure was initially performed in 1968 by Francis Fontan and Eugene Baudet from Bordeaux, France, published in 1971, simultaneously described in July 1971 by Guillermo Kreutzer from Buenos Aires, Argentina, presented at the Argentinean National Cardilogy meeting of that year and finally published in 1973.
Situs ambiguus is a rare congenital defect in which the major visceral organs are distributed abnormally within the chest and abdomen. Clinically heterotaxy spectrum generally refers to any defect of Left-right asymmetry and arrangement of the visceral organs; however, classical heterotaxy requires multiple organs to be affected. This does not include the congenital defect situs inversus, which results when arrangement of all the organs in the abdomen and chest are mirrored, so the positions are opposite the normal placement. Situs inversus is the mirror image of situs solitus, which is normal asymmetric distribution of the abdominothoracic visceral organs. Situs ambiguus can also be subdivided into left-isomerism and right isomerism based on the defects observed in the spleen, lungs and atria of the heart.

The jugular veins are veins that take blood from the head back to the heart via the superior vena cava. The internal jugular vein descends next to the internal carotid artery and continues posteriorly to the sternocleidomastoid muscle.
The atrium is one of the two upper chambers in the heart that receives blood from the circulatory system. The blood in the atria is pumped into the heart ventricles through the atrioventricular mitral and tricuspid heart valves.

A pulmonary sequestration is a medical condition wherein a piece of tissue that ultimately develops into lung tissue is not attached to the pulmonary arterial blood supply, as is the case in normally developing lung. This sequestered tissue is therefore not connected to the normal bronchial airway architecture, and fails to function in, and contribute to, respiration of the organism.

Pulmonary angiography is a medical fluoroscopic procedure used to visualize the pulmonary arteries and much less frequently, the pulmonary veins. It is a minimally invasive procedure performed most frequently by an interventional radiologist or interventional cardiologist to visualise the arteries of the lungs.

An inferior vena cava filter is a medical device made of metal that is implanted by vascular surgeons or interventional radiologists into the inferior vena cava to prevent a life-threatening pulmonary embolism (PE) or venous thromboembolism (VTE).

The coronary sinus is the largest vein of the heart. It drains over half of the deoxygenated blood from the heart muscle into the right atrium. It begins on the backside of the heart, in between the left atrium, and left ventricle; it begins at the junction of the great cardiac vein, and oblique vein of the left atrium. It receives multiple tributaries. It passes across the backside of the heart along a groove between left atrium and left ventricle, then drains into the right atrium at the orifice of the coronary sinus.

An umbilical line is a catheter that is inserted into one of the two arteries or the vein of the umbilical cord. Generally the UAC/UVC is used in Neonatal Intensive Care Units (NICU) as it provides quick access to the central circulation of premature infants. UAC/UVC lines can be placed at the time of birth and allow medical staff to quickly infuse fluids, inotropic drugs, and blood if required. It is sometimes used in term or near-term newborns in whom the umbilical cord stump is still connected to the circulatory system. Medications, fluids, and blood can be given through this catheter and it allows monitoring of blood gasses and withdrawing of blood samples. Transumbilical catheter intervention is also a method of gaining access to the heart, for example to surgically correct a patent ductus arteriosus.
Venous return is the rate of blood flow back to the heart. It normally limits cardiac output.

Anomalous pulmonary venous connection is a congenital defect of the pulmonary veins.
Congenital stenosis of vena cava is a congenital anomaly in which the superior vena cava or inferior vena cava has an aberrant interruption or coarctation.
Raghib syndrome is rare a congenital heart defect where the left superior vena cava (LSVC) is draining into the left atrium in addition to an absent coronary sinus and an atrial septal defect. This can be considered a dangerous heart condition because it puts the individual at a high risk of stroke. Other defects that are often associated with Raghib syndrome can include ventricular septal defects, enlargement of the tricuspid annulus, and pulmonary stenosis. While this is considered an extremely rare developmental complex, cases regarding a persistent left superior vena cava (PLSVC) are relatively common among congenital heart defects. It is also important to note that the PLSVC often drains into the right atrium, and only drains into the left atrium in approximately 10 to 20% of individuals with the defect.

