
Cardiac arrest, also known as sudden cardiac arrest, is when the heart suddenly and unexpectedly stops beating. As a result, blood cannot properly circulate around the body and there is diminished blood flow to the brain and other organs. When the brain does not receive enough blood, this can cause a person to lose consciousness. Coma and persistent vegetative state may result from cardiac arrest. Cardiac arrest is also identified by a lack of central pulses and abnormal or absent breathing.

Cardiopulmonary resuscitation (CPR) is an emergency procedure consisting of chest compressions often combined with artificial ventilation, or mouth to mouth in an effort to manually preserve intact brain function until further measures are taken to restore spontaneous blood circulation and breathing in a person who is in cardiac arrest. It is recommended for those who are unresponsive with no breathing or abnormal breathing, for example, agonal respirations.

Advanced cardiac life support, advanced cardiovascular life support (ACLS) refers to a set of clinical guidelines established by the American Heart Association (AHA) for the urgent and emergent treatment of life-threatening cardiovascular conditions that will cause or have caused cardiac arrest, using advanced medical procedures, medications, and techniques. ACLS expands on Basic Life Support (BLS) by adding recommendations on additional medication and advanced procedure use to the CPR guidelines that are fundamental and efficacious in BLS. ACLS is practiced by advanced medical providers including physicians, some nurses and paramedics; these providers are usually required to hold certifications in ACLS care.

Defibrillation is a treatment for life-threatening cardiac arrhythmias, specifically ventricular fibrillation (V-Fib) and non-perfusing ventricular tachycardia (V-Tach). A defibrillator delivers a dose of electric current to the heart. Although not fully understood, this process depolarizes a large amount of the heart muscle, ending the arrhythmia. Subsequently, the body's natural pacemaker in the sinoatrial node of the heart is able to re-establish normal sinus rhythm. A heart which is in asystole (flatline) cannot be restarted by a defibrillator; it would be treated only by cardiopulmonary resuscitation (CPR) and medication, and then by cardioversion or defibrillation if it converts into a shockable rhythm.

Asystole is the absence of ventricular contractions in the context of a lethal heart arrhythmia. Asystole is the most serious form of cardiac arrest and is usually irreversible. Also referred to as cardiac flatline, asystole is the state of total cessation of electrical activity from the heart, which means no tissue contraction from the heart muscle and therefore no blood flow to the rest of the body.
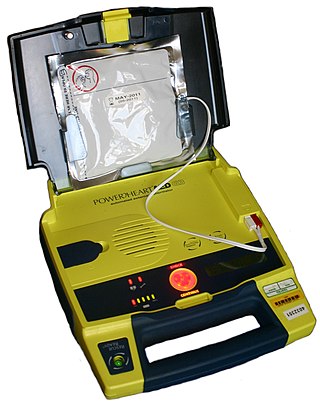
An automated external defibrillator or automatic electronic defibrillator (AED) is a portable electronic device that automatically diagnoses the life-threatening cardiac arrhythmias of ventricular fibrillation (VF) and pulseless ventricular tachycardia, and is able to treat them through defibrillation, the application of electricity which stops the arrhythmia, allowing the heart to re-establish an effective rhythm.
Basic life support (BLS) is a level of medical care which is used for patients with life-threatening condition of cardiac arrest until they can be given full medical care by advanced life support providers. It can be provided by trained medical personnel, such as emergency medical technicians, qualified bystanders and anybody who is trained for providing BLS and/or ACLS.
The Seattle & King County Emergency Medical Services System is a fire-based two-tier response system providing prehospital basic and advanced life support services.

Traumatic cardiac arrest (TCA) is a condition in which the heart has ceased to beat due to blunt or penetrating trauma, such as a stab wound to the thoracic area. It is a medical emergency which will always result in death without prompt advanced medical care. Even with prompt medical intervention, survival without neurological complications is rare. In recent years, protocols have been proposed to improve survival rate in patients with traumatic cardiac arrest, though the variable causes of this condition as well as many coexisting injuries can make these protocols difficult to standardize. Traumatic cardiac arrest is a complex form of cardiac arrest often derailing from advanced cardiac life support in the sense that the emergency team must first establish the cause of the traumatic arrest and reverse these effects, for example hypovolemia and haemorrhagic shock due to a penetrating injury.
Pulseless electrical activity (PEA) is a form of cardiac arrest in which the electrocardiogram shows a heart rhythm that should produce a pulse, but does not. Pulseless electrical activity is found initially in about 20% of out-of-hospital cardiac arrests and about 50% of in-hospital cardiac arrests.

Advanced Life Support (ALS) is a set of life saving protocols and skills that extend basic life support to further support the circulation and provide an open airway and adequate ventilation (breathing).

ABC and its variations are initialism mnemonics for essential steps used by both medical professionals and lay persons when dealing with a patient. In its original form it stands for Airway, Breathing, and Circulation. The protocol was originally developed as a memory aid for rescuers performing cardiopulmonary resuscitation, and the most widely known use of the initialism is in the care of the unconscious or unresponsive patient, although it is also used as a reminder of the priorities for assessment and treatment of patients in many acute medical and trauma situations, from first-aid to hospital medical treatment. Airway, breathing, and circulation are all vital for life, and each is required, in that order, for the next to be effective: a viable Airway is necessary for Breathing to provide oxygenated blood for Circulation. Since its development, the mnemonic has been extended and modified to fit the different areas in which it is used, with different versions changing the meaning of letters or adding other letters.
The chain of survival refers to a series of actions that, properly executed, reduce the mortality associated with sudden cardiac arrest. Like any chain, the chain of survival is only as strong as its weakest link. The six interdependent links in the chain of survival are early recognition of sudden cardiac arrest and access to emergency medical care, early CPR, early defibrillation, early advanced cardiac life support, and physical and emotional recovery. The first three links in the chain can be performed by lay bystanders, while the second three links are designated to medical professionals. Currently, between 70 and 90% of cardiac arrest patients die before they reach the hospital. However, a cardiac arrest does not have to be lethal if bystanders can take the right steps immediately.
The history of cardiopulmonary resuscitation (CPR) can be traced as far back as the literary works of ancient Egypt. However, it was not until the 18th century that credible reports of cardiopulmonary resuscitation began to appear in the medical literature.
Lazarus syndrome, also known as autoresuscitation after failed cardiopulmonary resuscitation, is the spontaneous return of a normal cardiac rhythm after failed attempts at resuscitation. It is also used to refer to the spontaneous return of cardiac activity after the patient has been pronounced dead. Its occurrence has been noted in medical literature at least 38 times since 1982. It takes its name from Lazarus who, according to the New Testament, was raised from the dead by Jesus.
Return of spontaneous circulation (ROSC) is the resumption of a sustained heart rhythm that perfuses the body after cardiac arrest. It is commonly associated with significant respiratory effort. Signs of return of spontaneous circulation include breathing, coughing, or movement and a palpable pulse or a measurable blood pressure. Someone is considered to have sustained return of spontaneous circulation when circulation persists and cardiopulmonary resuscitation has ceased for at least 20 consecutive minutes.
An inspiratory impedance threshold device is a valve used in cardiopulmonary resuscitation (CPR) to decrease intrathoracic pressure and improve venous return to the heart. The valve is a part of a mask or other breathing device such as an endotracheal tube, and may open at high or low pressures

Rearrest is a phenomenon that involves the resumption of a lethal cardiac dysrhythmia after successful return of spontaneous circulation (ROSC) has been achieved during the course of resuscitation. Survival to hospital discharge rates are as low as 7% for cardiac arrest in general and although treatable, rearrest may worsen these survival chances. Rearrest commonly occurs in the out-of-hospital setting under the treatment of health care providers.
Extracorporeal cardiopulmonary resuscitation is a method of cardiopulmonary resuscitation (CPR) that passes the patient's blood through a machine in a process to oxygenate the blood supply. A portable extracorporeal membrane oxygenation (ECMO) device is used as an adjunct to standard CPR. A patient who is deemed to be in cardiac arrest refractory to CPR has percutaneous catheters inserted into the femoral vein and artery. Theoretically, the application of ECPR allows for the return of cerebral perfusion in a more sustainable manner than with external compressions alone. By attaching an ECMO device to a person who has acutely undergone cardiovascular collapse, practitioners can maintain end-organ perfusion whilst assessing the potential reversal of causal pathology, with the goal of improving long-term survival and neurological outcomes.

The Lund University Cardiopulmonary Assist System (LUCAS) device provides mechanical chest compressions to patients in cardiac arrest. It is mostly used in emergency medicine as an alternative to manual CPR because it provides consistent compressions at a fixed rate through difficult transport conditions and eliminates the physical strain on the person performing CPR. The first generation of the LUCAS device was pneumatic, while the second and third generations are battery-operated.



