
Benign nephrosclerosis refers to the renal changes most commonly occurring in association with long-standing hypertension. It is termed benign because it rarely progresses to clinically significant chronic kidney disease or kidney failure. [1]
Benign nephrosclerosis refers to the renal changes most commonly occurring in association with long-standing hypertension. It is termed benign because it rarely progresses to clinically significant chronic kidney disease or kidney failure. [1]
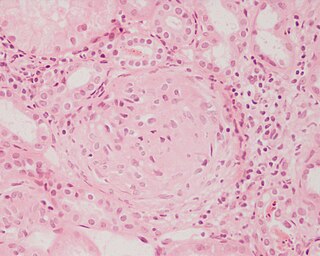
The kidneys appear symmetrically atrophic and there is a reduced nephron mass. [1] The kidneys have a surface of diffuse, fine granularity that resembles grain leather. Microscopically, the basic anatomic change consists of hyaline thickening of the walls of the small arteries and arterioles (hyaline arteriolosclerosis). Under a microscope, this appears as a homogeneous, pink hyaline thickening at the expense of the vessel lumina, with loss of underlying cellular detail. The narrowing of the lumen restricts blood flow, resulting in ischemia. All structures of the kidney can show ischemic atrophy although glomerular ischemic atrophy may be patchy. [1] In advanced cases of benign nephrosclerosis the glomerular tufts may become globally sclerosed. Diffuse tubular atrophy and interstitial fibrosis are present. Often there is a scant interstitial lymphocytic infiltrate. The larger blood vessels (interlobar and arcuate arteries) show reduplication of internal elastic lamina along with fibrous thickening of the media (fibroelastic hyperplasia) and the subintima. [1]
Benign nephrosclerosis alone hardly ever causes severe damage to the kidney, except in susceptible populations, such as African Americans, where it may lead to uremia and death. However, all persons with this disease usually show some functional impairment, such as loss of concentration or a variably diminished GFR. A mild degree of proteinuria is a frequent finding. [2]

In humans, the kidneys are two reddish-brown bean-shaped blood-filtering organs that are a multilobar, multipapillary form of mammalian kidneys, usually without signs of external lobulation. They are located on the left and right in the retroperitoneal space, and in adult humans are about 12 centimetres in length. They receive blood from the paired renal arteries; blood exits into the paired renal veins. Each kidney is attached to a ureter, a tube that carries excreted urine to the bladder.
Azotemia is a medical condition characterized by abnormally high levels of nitrogen-containing compounds in the blood. It is largely related to insufficient or dysfunctional filtering of blood by the kidneys. It can lead to uremia and acute kidney injury if not controlled.

The nephron is the minute or microscopic structural and functional unit of the kidney. It is composed of a renal corpuscle and a renal tubule. The renal corpuscle consists of a tuft of capillaries called a glomerulus and a cup-shaped structure called Bowman's capsule. The renal tubule extends from the capsule. The capsule and tubule are connected and are composed of epithelial cells with a lumen. A healthy adult has 1 to 1.5 million nephrons in each kidney. Blood is filtered as it passes through three layers: the endothelial cells of the capillary wall, its basement membrane, and between the foot processes of the podocytes of the lining of the capsule. The tubule has adjacent peritubular capillaries that run between the descending and ascending portions of the tubule. As the fluid from the capsule flows down into the tubule, it is processed by the epithelial cells lining the tubule: water is reabsorbed and substances are exchanged ; first with the interstitial fluid outside the tubules, and then into the plasma in the adjacent peritubular capillaries through the endothelial cells lining that capillary. This process regulates the volume of body fluid as well as levels of many body substances. At the end of the tubule, the remaining fluid—urine—exits: it is composed of water, metabolic waste, and toxins.

Nephritis is inflammation of the kidneys and may involve the glomeruli, tubules, or interstitial tissue surrounding the glomeruli and tubules. It is one of several different types of nephropathy.

Ischemia or ischaemia is a restriction in blood supply to any tissue, muscle group, or organ of the body, causing a shortage of oxygen that is needed for cellular metabolism. Ischemia is generally caused by problems with blood vessels, with resultant damage to or dysfunction of tissue i.e. hypoxia and microvascular dysfunction. It also implies local hypoxia in a part of a body resulting from constriction.
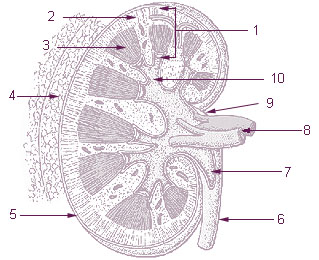
The renal medulla is the innermost part of the kidney. The renal medulla is split up into a number of sections, known as the renal pyramids. Blood enters into the kidney via the renal artery, which then splits up to form the segmental arteries which then branch to form interlobar arteries. The interlobar arteries each in turn branch into arcuate arteries, which in turn branch to form interlobular arteries, and these finally reach the glomeruli. At the glomerulus the blood reaches a highly disfavourable pressure gradient and a large exchange surface area, which forces the serum portion of the blood out of the vessel and into the renal tubules. Flow continues through the renal tubules, including the proximal tubule, the loop of Henle, through the distal tubule and finally leaves the kidney by means of the collecting duct, leading to the renal pelvis, the dilated portion of the ureter.

Polyarteritis nodosa (PAN) is a systemic necrotizing inflammation of blood vessels (vasculitis) affecting medium-sized muscular arteries, typically involving the arteries of the kidneys and other internal organs but generally sparing the lungs' circulation. Small aneurysms are strung like the beads of a rosary, therefore making this "rosary sign" an important diagnostic feature of the vasculitis. PAN is sometimes associated with infection by the hepatitis B or hepatitis C virus. The condition may be present in infants.
Glomerulonephritis (GN) is a term used to refer to several kidney diseases. Many of the diseases are characterised by inflammation either of the glomeruli or of the small blood vessels in the kidneys, hence the name, but not all diseases necessarily have an inflammatory component.

Renal artery stenosis (RAS) is the narrowing of one or both of the renal arteries, most often caused by atherosclerosis or fibromuscular dysplasia. This narrowing of the renal artery can impede blood flow to the target kidney, resulting in renovascular hypertension – a secondary type of high blood pressure. Possible complications of renal artery stenosis are chronic kidney disease and coronary artery disease.

Hypertensive kidney disease is a medical condition referring to damage to the kidney due to chronic high blood pressure. It manifests as hypertensive nephrosclerosis. It should be distinguished from renovascular hypertension, which is a form of secondary hypertension, and thus has opposite direction of causation.

Arteriolosclerosis is a form of cardiovascular disease involving hardening and loss of elasticity of arterioles or small arteries and is most often associated with hypertension and diabetes mellitus. Types include hyaline arteriolosclerosis and hyperplastic arteriolosclerosis, both involved with vessel wall thickening and luminal narrowing that may cause downstream ischemic injury. The following two terms whilst similar, are distinct in both spelling and meaning and may easily be confused with arteriolosclerosis.
The myogenic mechanism is how arteries and arterioles react to an increase or decrease of blood pressure to keep the blood flow constant within the blood vessel. Myogenic response refers to a contraction initiated by the myocyte itself instead of an outside occurrence or stimulus such as nerve innervation. Most often observed in smaller resistance arteries, this 'basal' myogenic tone may be useful in the regulation of organ blood flow and peripheral resistance, as it positions a vessel in a preconstricted state that allows other factors to induce additional constriction or dilation to increase or decrease blood flow.

Cholesterol embolism occurs when cholesterol is released, usually from an atherosclerotic plaque, and travels as an embolus in the bloodstream to lodge causing an obstruction in blood vessels further away. Most commonly this causes skin symptoms, gangrene of the extremities and sometimes kidney failure; problems with other organs may arise, depending on the site at which the cholesterol crystals enter the bloodstream. When the kidneys are involved, the disease is referred to as atheroembolic renal disease. The diagnosis usually involves biopsy from an affected organ. Cholesterol embolism is treated by removing the cause and giving supportive therapy; statin drugs have been found to improve the prognosis.
Diffuse proliferative glomerulonephritis (DPGN) is a type of glomerulonephritis that is the most serious form of renal lesions in SLE and is also the most common, occurring in 35% to 60% of patients. In absence of SLE, DPGN pathology looks more like Membranoproliferative glomerulonephritis
Sickle cell nephropathy is a type of nephropathy associated with sickle cell disease which causes kidney complications as a result of sickling of red blood cells in the small blood vessels. The hypertonic and relatively hypoxic environment of the renal medulla, coupled with the slow blood flow in the vasa recta, favors sickling of red blood cells, with resultant local infarction. Functional tubule defects in patients with sickle cell disease are likely the result of partial ischemic injury to the renal tubules.

Complications of hypertension are clinical outcomes that result from persistent elevation of blood pressure. Hypertension is a risk factor for all clinical manifestations of atherosclerosis since it is a risk factor for atherosclerosis itself. It is an independent predisposing factor for heart failure, coronary artery disease, stroke, kidney disease, and peripheral arterial disease. It is the most important risk factor for cardiovascular morbidity and mortality, in industrialized countries.
Glomerulocystic kidney disease (GCKD) is a cystic disorder of the kidneys. GCKD involves cystic dilation of Bowman's capsule. It can occur with or without congenital abnormality.

Renal ultrasonography is the examination of one or both kidneys using medical ultrasound.
Kidney ischemia is a disease with a high morbidity and mortality rate. Blood vessels shrink and undergo apoptosis which results in poor blood flow in the kidneys. More complications happen when failure of the kidney functions result in toxicity in various parts of the body which may cause septic shock, hypovolemia, and a need for surgery. What causes kidney ischemia is not entirely known, but several pathophysiology relating to this disease have been elucidated. Possible causes of kidney ischemia include the activation of IL-17C and hypoxia due to surgery or transplant. Several signs and symptoms include injury to the microvascular endothelium, apoptosis of kidney cells due to overstress in the endoplasmic reticulum, dysfunctions of the mitochondria, autophagy, inflammation of the kidneys, and maladaptive repair.

The mammalian kidneys are a pair of excretory organs of the urinary system of mammals, being functioning kidneys in postnatal-to-adult individuals. The kidneys in mammals are usually bean-shaped or externally lobulated. They are located behind the peritoneum (retroperitoneally) on the back (dorsal) wall of the body. The typical mammalian kidney consists of a renal capsule, a peripheral cortex, an internal medulla, one or more renal calyces, and a renal pelvis. Although the calyces or renal pelvis may be absent in some species. The medulla is made up of one or more renal pyramids, forming papillae with their innermost parts. Generally, urine produced by the cortex and medulla drains from the papillae into the calyces, and then into the renal pelvis, from which urine exits the kidney through the ureter. Nitrogen-containing waste products are excreted by the kidneys in mammals mainly in the form of urea.