
The humerus is a long bone in the arm that runs from the shoulder to the elbow. It connects the scapula and the two bones of the lower arm, the radius and ulna, and consists of three sections. The humeral upper extremity consists of a rounded head, a narrow neck, and two short processes. The body is cylindrical in its upper portion, and more prismatic below. The lower extremity consists of 2 epicondyles, 2 processes, and 3 fossae. As well as its true anatomical neck, the constriction below the greater and lesser tubercles of the humerus is referred to as its surgical neck due to its tendency to fracture, thus often becoming the focus of surgeons.
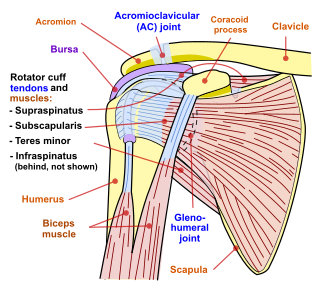
The rotator cuff is a group of muscles and their tendons that act to stabilize the human shoulder and allow for its extensive range of motion. Of the seven scapulohumeral muscles, four make up the rotator cuff. The four muscles are:
Shoulder problems including pain, are one of the more common reasons for physician visits for musculoskeletal symptoms. The shoulder is the most movable joint in the body. However, it is an unstable joint because of the range of motion allowed. This instability increases the likelihood of joint injury, often leading to a degenerative process in which tissues break down and no longer function well.

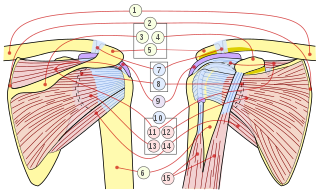
The human shoulder is made up of three bones: the clavicle (collarbone), the scapula, and the humerus as well as associated muscles, ligaments and tendons.

The deltoid muscle is the muscle forming the rounded contour of the human shoulder. It is also known as the 'common shoulder muscle', particularly in other animals such as the domestic cat. Anatomically, the deltoid muscle appears to be made up of three distinct sets of muscle fibers, namely the
- anterior or clavicular part
- posterior or scapular part
- intermediate or acromial part
Rotator cuff tendinopathy is a process of senescence. The pathophysiology is mucoid degeneration. Most people develop rotator cuff tendinopathy within their lifetime.

The teres minor is a narrow, elongated muscle of the rotator cuff. The muscle originates from the lateral border and adjacent posterior surface of the corresponding right or left scapula and inserts at both the greater tubercle of the humerus and the posterior surface of the joint capsule.

The supraspinatus is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.

In human anatomy, the infraspinatus muscle is a thick triangular muscle, which occupies the chief part of the infraspinatous fossa. As one of the four muscles of the rotator cuff, the main function of the infraspinatus is to externally rotate the humerus and stabilize the shoulder joint.

The shoulder joint is structurally classified as a synovial ball-and-socket joint and functionally as a diarthrosis and multiaxial joint. It involves an articulation between the glenoid fossa of the scapula and the head of the humerus. Due to the very loose joint capsule that gives a limited interface of the humerus and scapula, it is the most mobile joint of the human body.

The subscapularis is a large triangular muscle which fills the subscapular fossa and inserts into the lesser tubercle of the humerus and the front of the capsule of the shoulder-joint.
In medicine, physiotherapy, chiropractic, and osteopathy the hip examination, or hip exam, is undertaken when a patient has a complaint of hip pain and/or signs and/or symptoms suggestive of hip joint pathology. It is a physical examination maneuver.
Subacromial bursitis is a condition caused by inflammation of the bursa that separates the superior surface of the supraspinatus tendon from the overlying coraco-acromial ligament, acromion, and coracoid and from the deep surface of the deltoid muscle. The subacromial bursa helps the motion of the supraspinatus tendon of the rotator cuff in activities such as overhead work.

Shoulder replacement is a surgical procedure in which all or part of the glenohumeral joint is replaced by a prosthetic implant. Such joint replacement surgery generally is conducted to relieve arthritis pain or fix severe physical joint damage.
Shoulder impingement syndrome is a syndrome involving tendonitis of the rotator cuff muscles as they pass through the subacromial space, the passage beneath the acromion. It is particularly associated with tendonitis of the supraspinatus muscle. This can result in pain, weakness, and loss of movement at the shoulder.
The Neer Impingement Test is a test designed to reproduce symptoms of rotator cuff impingement through flexing the shoulder and pressure application. Symptoms should be reproduced if there is a problem with the supraspinatus or biceps brachii. This test is also associated with the Hawkins-Kennedy Test and Jobe's Test.
Jobe's test, also known as empty can test, is an orthopedic examination used to test stability of the shoulder.
A shoulder examination is a portion of a physical examination used to identify potential pathology involving the shoulder. It should be conducted with both shoulders exposed to assess for asymmetry and muscle wasting.
Yergason's test is a special test used for orthopedic examination of the shoulder and upper arm region, specifically the biceps tendon.
The Hawkins–Kennedy Test is a test used in the evaluation of orthopedic shoulder injury. It was first described in the 1980s by Canadian Drs. R. Hawkins and J. Kennedy, and a positive test is most likely indicative of damage to the tendon of the supraspinatus muscle.