| Supraspinatus muscle | |
|---|---|
 Position of the supraspinatus muscle (red) seen from the back. | |
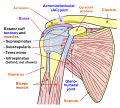
 Posterior view of muscles connecting the upper extremity to the vertebral column. Supraspinatus muscle is labeled in red at right, while it is covered by other muscles at left. | |
| Details | |
| Origin | Supraspinous fossa of scapula |
| Insertion | Superior facet of greater tubercle of humerus |
| Artery | Suprascapular artery |
| Nerve | Suprascapular nerve |
| Actions | Abduction of arm and stabilizes humerus |
| Identifiers | |
| Latin | musculus supraspinatus |
| TA98 | A04.6.02.006 |
| TA2 | 2457 |
| FMA | 9629 |
| Anatomical terms of muscle | |
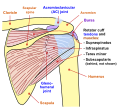
The supraspinatus (pl.: supraspinati) is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula (shoulder blade) to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.