
In human anatomy, the arm refers to the upper limb in common usage, although academically the term specifically means the upper arm between the glenohumeral joint and the elbow joint. The distal part of the upper limb between the elbow and the radiocarpal joint is known as the forearm or "lower" arm, and the extremity beyond the wrist is the hand.

The humerus is a long bone in the arm that runs from the shoulder to the elbow. It connects the scapula and the two bones of the lower arm, the radius and ulna, and consists of three sections. The humeral upper extremity consists of a rounded head, a narrow neck, and two short processes. The body is cylindrical in its upper portion, and more prismatic below. The lower extremity consists of 2 epicondyles, 2 processes, and 3 fossae. As well as its true anatomical neck, the constriction below the greater and lesser tubercles of the humerus is referred to as its surgical neck due to its tendency to fracture, thus often becoming the focus of surgeons.

The radial nerve is a nerve in the human body that supplies the posterior portion of the upper limb. It innervates the medial and lateral heads of the triceps brachii muscle of the arm, as well as all 12 muscles in the posterior osteofascial compartment of the forearm and the associated joints and overlying skin.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.

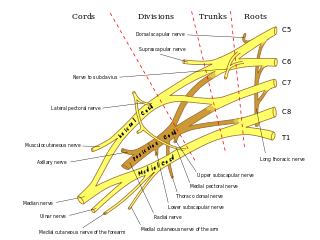
The brachial plexus is a network of nerves formed by the anterior rami of the lower four cervical nerves and first thoracic nerve. This plexus extends from the spinal cord, through the cervicoaxillary canal in the neck, over the first rib, and into the armpit, it supplies afferent and efferent nerve fibers to the chest, shoulder, arm, forearm, and hand.
Pronator quadratus is a square-shaped muscle on the distal forearm that acts to pronate the hand.
The forearm is the region of the upper limb between the elbow and the wrist. The term forearm is used in anatomy to distinguish it from the arm, a word which is used to describe the entire appendage of the upper limb, but which in anatomy, technically, means only the region of the upper arm, whereas the lower "arm" is called the forearm. It is homologous to the region of the leg that lies between the knee and the ankle joints, the crus.
The ulnar nerve is a nerve that runs near the ulna, one of the two long bones in the forearm. The ulnar collateral ligament of elbow joint is in relation with the ulnar nerve. The nerve is the largest in the human body unprotected by muscle or bone, so injury is common. This nerve is directly connected to the little finger, and the adjacent half of the ring finger, innervating the palmar aspect of these fingers, including both front and back of the tips, perhaps as far back as the fingernail beds.

The upper limbs or upper extremities are the forelimbs of an upright-postured tetrapod vertebrate, extending from the scapulae and clavicles down to and including the digits, including all the musculatures and ligaments involved with the shoulder, elbow, wrist and knuckle joints. In humans, each upper limb is divided into the shoulder, arm, elbow, forearm, wrist and hand, and is primarily used for climbing, lifting and manipulating objects. In anatomy, just as arm refers to the upper arm, leg refers to the lower leg.
The musculocutaneous nerve is a mixed branch of the lateral cord of the brachial plexus derived from cervical spinal nerves C5-C7. It arises opposite the lower border of the pectoralis major. It provides motor innervation to the muscles of the anterior compartment of the arm: the coracobrachialis, biceps brachii, and brachialis. It provides sensory innervation to the lateral forearm. It courses through the anterior part of the arm, terminating 2 cm above elbow; after passing the lateral edge of the tendon of biceps brachii it is becomes known as the lateral cutaneous nerve of the forearm.
The cubital fossa, antecubital fossa, chelidon, or inside of elbow is the area on the anterior side of the upper part between the arm and forearm of a human or other hominid animals. It lies anteriorly to the elbow (antecubital) when in standard anatomical position. The cubital fossa is a triangular area having three borders.

The ulnar artery is the main blood vessel, with oxygenated blood, of the medial aspects of the forearm. It arises from the brachial artery and terminates in the superficial palmar arch, which joins with the superficial branch of the radial artery. It is palpable on the anterior and medial aspect of the wrist.
The flexor pollicis longus is a muscle in the forearm and hand that flexes the thumb. It lies in the same plane as the flexor digitorum profundus. This muscle is unique to humans, being either rudimentary or absent in other primates. A meta-analysis indicated accessory flexor pollicis longus is present in around 48% of the population.

In human anatomy, the supinator is a broad muscle in the posterior compartment of the forearm, curved around the upper third of the radius. Its function is to supinate the forearm.
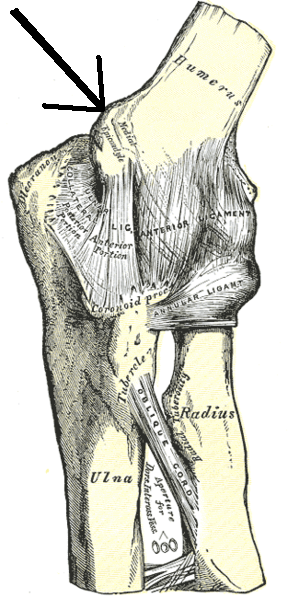
The medial epicondyle of the humerus is an epicondyle of the humerus bone of the upper arm in humans. It is larger and more prominent than the lateral epicondyle and is directed slightly more posteriorly in the anatomical position. In birds, where the arm is somewhat rotated compared to other tetrapods, it is called the ventral epicondyle of the humerus. In comparative anatomy, the more neutral term entepicondyle is used.
Golfer's elbow, or medial epicondylitis, is tendinosis of the medial common flexor tendon on the inside of the elbow. It is similar to tennis elbow, which affects the outside of the elbow at the lateral epicondyle. The tendinopathy results from overload or repetitive use of the arm, causing an injury similar to ulnar collateral ligament injury of the elbow in "pitcher's elbow".

The fascial compartments of arm refers to the specific anatomical term of the compartments within the upper segment of the upper limb of the body. The upper limb is divided into two segments, the arm and the forearm. Each of these segments is further divided into two compartments which are formed by deep fascia – tough connective tissue septa (walls). Each compartment encloses specific muscles and nerves.

The cervical spinal nerve 8 (C8) is a spinal nerve of the cervical segment.

A supracondylar humerus fracture is a fracture of the distal humerus just above the elbow joint. The fracture is usually transverse or oblique and above the medial and lateral condyles and epicondyles. This fracture pattern is relatively rare in adults, but is the most common type of elbow fracture in children. In children, many of these fractures are non-displaced and can be treated with casting. Some are angulated or displaced and are best treated with surgery. In children, most of these fractures can be treated effectively with expectation for full recovery. Some of these injuries can be complicated by poor healing or by associated blood vessel or nerve injuries with serious complications.
Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.




