Related Research Articles
Lung cancer, also known as lung carcinoma, is a malignant tumor that begins in the lung. Lung cancer is caused by genetic damage to the DNA of cells in the airways, often caused by cigarette smoking or inhaling damaging chemicals. Damaged airway cells gain the ability to multiply unchecked, causing the growth of a tumor. Without treatment, tumors spread throughout the lung, damaging lung function. Eventually lung tumors metastasize, spreading to other parts of the body.

Cytopathology is a branch of pathology that studies and diagnoses diseases on the cellular level. The discipline was founded by George Nicolas Papanicolaou in 1928. Cytopathology is generally used on samples of free cells or tissue fragments, in contrast to histopathology, which studies whole tissues. Cytopathology is frequently, less precisely, called "cytology", which means "the study of cells".

Pulmonology, pneumology or pneumonology is a medical specialty that deals with diseases involving the respiratory tract. It is also known as respirology, respiratory medicine, or chest medicine in some countries and areas.

Lymphadenopathy or adenopathy is a disease of the lymph nodes, in which they are abnormal in size or consistency. Lymphadenopathy of an inflammatory type is lymphadenitis, producing swollen or enlarged lymph nodes. In clinical practice, the distinction between lymphadenopathy and lymphadenitis is rarely made and the words are usually treated as synonymous. Inflammation of the lymphatic vessels is known as lymphangitis. Infectious lymphadenitis affecting lymph nodes in the neck is often called scrofula.

Miliary tuberculosis is a form of tuberculosis that is characterized by a wide dissemination into the human body and by the tiny size of the lesions (1–5 mm). Its name comes from a distinctive pattern seen on a chest radiograph of many tiny spots distributed throughout the lung fields with the appearance similar to millet seeds—thus the term "miliary" tuberculosis. Miliary TB may infect any number of organs, including the lungs, liver, and spleen. Miliary tuberculosis is present in about 2% of all reported cases of tuberculosis and accounts for up to 20% of all extra-pulmonary tuberculosis cases.

A chylothorax is an abnormal accumulation of chyle, a type of lipid-rich lymph, in the space surrounding the lung. The lymphatics of the digestive system normally returns lipids absorbed from the small bowel via the thoracic duct, which ascends behind the esophagus to drain into the left brachiocephalic vein. If normal thoracic duct drainage is disrupted, either due to obstruction or rupture, chyle can leak and accumulate within the negative-pressured pleural space. In people on a normal diet, this fluid collection can sometimes be identified by its turbid, milky white appearance, since chyle contains emulsified triglycerides.
ICD-9-CM Volume 3 is a system of procedural codes used by health insurers to classify medical procedures for billing purposes. It is a subset of the International Statistical Classification of Diseases and Related Health Problems (ICD) 9-CM. Volumes 1 and 2 are used for diagnostic codes.
Bronchoalveolar lavage (BAL) is a diagnostic method of the lower respiratory system in which a bronchoscope is passed through the mouth or nose into an appropriate airway in the lungs, with a measured amount of fluid introduced and then collected for examination. This method is typically performed to diagnose pathogenic infections of the lower respiratory airways, though it also has been shown to have utility in diagnosing interstitial lung disease. Bronchoalveolar lavage can be a more sensitive method of detection than nasal swabs in respiratory molecular diagnostics, as has been the case with SARS-CoV-2 where bronchoalveolar lavage samples detect copies of viral RNA after negative nasal swab testing.

Endoscopic ultrasound (EUS) or echo-endoscopy is a medical procedure in which endoscopy is combined with ultrasound to obtain images of the internal organs in the chest, abdomen and colon. It can be used to visualize the walls of these organs, or to look at adjacent structures. Combined with Doppler imaging, nearby blood vessels can also be evaluated.

A mediastinal tumor is a tumor in the mediastinum, the cavity that separates the lungs from the rest of the chest. It contains the heart, esophagus, trachea, thymus, and aorta. The most common mediastinal masses are neurogenic tumors, usually found in the posterior mediastinum, followed by thymoma (15–20%) located in the anterior mediastinum. Lung cancer typically spreads to the lymph nodes in the mediastinum.
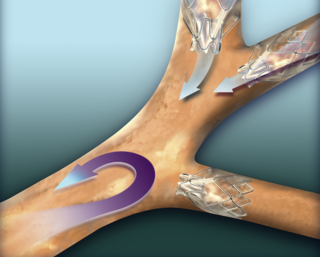
An endobronchial valve(EBV), is a small, one-way valve, which may be implanted in an airway feeding the lung or part of lung. The valve allows air to be breathed out of the section of lung supplied, and prevents air from being breathed in. This leaves the rest of the lung to expand more normally and avoid air-trapping. Endobronchial valves are typically implanted using a flexible delivery catheter advanced through a bronchoscope in minimally invasive bronchoscopic lung volume reduction procedures in the treatment of severe emphysema. The valves are also removable if they are not working properly.

Bronchoscopy is an endoscopic technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. An instrument (bronchoscope) is inserted into the airways, usually through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs. The construction of bronchoscopes ranges from rigid metal tubes with attached lighting devices to flexible optical fiber instruments with realtime video equipment.
Bronchial thermoplasty is a treatment for severe asthma approved by the FDA in 2010 involving the delivery of controlled, therapeutic radiofrequency energy to the airway wall, thus heating the tissue and reducing the amount of smooth muscle present in the airway wall. This reduces the capacity of the immune system to cause bronchoconstriction through nitric oxide signalling, which is the main root cause of asthma symptoms. Bronchial thermoplasty is normally used to treat patients with severe persistent asthma who do not respond well to typical pharmacotherapy regimens.
Lung cancer staging is the assessment of the extent to which a lung cancer has spread from its original source. As with most cancers, staging is an important determinant of treatment and prognosis. In general, more advanced stages of cancer are less amenable to treatment and have a worse prognosis.

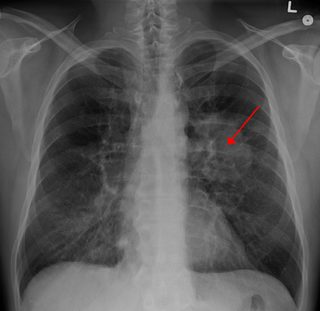
A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.
Bronchial brushing is a procedure in which cells are taken from the inside of the airway mucosa or bronchial lesions through catheter-based brushing under direct visualization or fluoroscopic guidance. Flexible brushes are passed through the bronchoscope, and the bronchial surface is gently abraded to obtain the specimen. Various types of bronchial brush may be used to collect both cellular and microbiological material, using direct vision when collecting from proximal areas of suspicion or fluoroscopic screening when sampling more peripheral sites. A bronchial brushing is used to find cancer and changes in cells that may lead to cancer. It can also be used to obtain specimens for microbiologic diagnosis.

Adenocarcinoma of the lung is the most common type of lung cancer, and like other forms of lung cancer, it is characterized by distinct cellular and molecular features. It is classified as one of several non-small cell lung cancers (NSCLC), to distinguish it from small cell lung cancer which has a different behavior and prognosis. Lung adenocarcinoma is further classified into several subtypes and variants. The signs and symptoms of this specific type of lung cancer are similar to other forms of lung cancer, and patients most commonly complain of persistent cough and shortness of breath.
Interventional pulmonology is a maturing medical sub-specialty from its parent specialty of pulmonary medicine. It deals specifically with minimally invasive endoscopic and percutaneous procedures for diagnosis and treatment of neoplastic as well as non-neoplastic diseases of the airways, lungs, and pleura. Many IP procedures constitute efficacious yet less invasive alternatives to thoracic surgery.

Pulmonary sclerosing pneumocytoma is a rare benign tumour of the lung.
Bronchoscopic lung volume reduction(BLVR) is a procedure to reduce the volume of air within the lungs. BLVR was initially developed in the early 2000s as a minimally invasive treatment for severe COPD that is primarily caused by emphysema. BLVR evolved from earlier surgical approaches first developed in the 1950s to reduce lung volume by removing damaged portions of the lungs via pneumonectomy or wedge resection. Procedures include the use of valves, coils, or thermal vapour ablation.
References
- 1 2 3 4 5 Reynisson, Pall J.; Leira, Håkon O.; Hernes, Toril N.; Hofstad, Erlend F.; Scali, Marta; Sorger, Hanne; Amundsen, Tore; Lindseth, Frank; Langø, Thomas (2014). "Navigated Bronchoscopy". Journal of Bronchology & Interventional Pulmonology. 21 (3): 242–264. doi: 10.1097/LBR.0000000000000064 . PMID 24992135. S2CID 31847196.
- 1 2 http://ajrccm.atsjournals.org/cgi/reprint/200603-344OCv1.pdf%5B%5D
- 1 2 3 4 Becker, Heinrich D.; Herth, Felix; Ernst, Armin; Schwarz, Yehuda (2005). "Bronchoscopic Biopsy of Peripheral Lung Lesions Under Electromagnetic Guidance". Journal of Bronchology. 12: 9–13. doi:10.1097/01.laboratory.0000147032.67754.22.
- ↑ "Electromagnetic Navigation-guided Bronchoscopy". aetna.com.
- ↑ Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M. J. (2007). "Cancer statistics, 2007". CA: A Cancer Journal for Clinicians. 57 (1): 43–66. doi: 10.3322/canjclin.57.1.43 . PMID 17237035. S2CID 22305510.
- ↑ American Cancer Society, 2006
- ↑ International Early Lung Cancer Action Program Investigators; Henschke, C. I.; Yankelevitz, D. F.; Libby, D. M.; Pasmantier, M. W.; Smith, J. P.; Miettinen, O. S. (2006). "Survival of Patients with Stage I Lung Cancer Detected on CT Screening". New England Journal of Medicine. 355 (17): 1763–1771. doi:10.1056/NEJMoa060476. PMID 17065637. S2CID 28552189.
- ↑ American Cancer Society, Surveillance Research, 2006
- ↑ "Homepage - American Lung Association". lungusa.org. Archived from the original on 2010-05-06. Retrieved 2022-01-10.
- ↑ US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General, 2004.
- ↑ Ernst, Armin; Silvestri, Gerard A.; Johnstone, David (2003). "Interventional Pulmonary Procedures". Chest. 123 (5): 1693–1694. doi: 10.1378/chest.123.5.1693 . ISSN 0012-3692. PMID 12740291. S2CID 39643448.
- ↑ Gildea, T; Mazzone, P; Karnak, D; Meziane, M; Mehta, A (2006). "Electromagnetic Navigation Diagnostic Bronchoscopy: A Prospective Study". American Journal of Respiratory and Critical Care Medicine. 174 (9): 982–989. doi:10.1164/rccm.200603-344oc. PMC 2648102 . PMID 16873767.
- ↑ Wilson, D; Bartlett, R (2007). "Improved Diagnostic Yield of Bronchoscopy in a Community practice: Combination of Electromagnetic Navigation System and Rapid On-Site Evaluation". Journal of Bronchology. 14 (4): 227–232. doi: 10.1097/lbr.0b013e31815a7b00 .
- ↑ Lamprecht, Bernd; Porsch, Peter; Pirich, Christian; Studnicka, Michael (2009). "Electromagnetic Navigation Bronchoscopy in Combination with PET-CT and Rapid On-site Cytopathologic Examination for Diagnosis of Peripheral Lung Lesions". Lung. 187 (1): 55–59. doi:10.1007/s00408-008-9120-8. PMID 18836886. S2CID 25076936.
- ↑ Gildea, Thomas R.; Mazzone, Peter J.; Karnak, Demet; Meziane, Moulay; Mehta, Atul C. (2006). "Electromagnetic Navigation Diagnostic Bronchoscopy". American Journal of Respiratory and Critical Care Medicine. 174 (9): 982–989. doi:10.1164/rccm.200603-344OC. PMC 2648102 . PMID 16873767.
- ↑ D. Makris (2007). "Electromagnetic navigation diagnostic bronchoscopy for small peripheral lung lesions". European Respiratory Journal. 29 (6): 1187–1192. doi: 10.1183/09031936.00165306 . PMID 17360724.
- ↑ O'Donoghue, Kilian; Eustace, David; Griffiths, James; O'Shea, Michael; Power, Timothy; Mansfield, Hilary; Cantillon-Murphy, Padraig (2014). "Catheter Position Tracking System Using Planar Magnetics and Closed Loop Current Control". IEEE Transactions on Magnetics. 50 (7): 1–9. Bibcode:2014ITM....5004271O. doi:10.1109/TMAG.2014.2304271. S2CID 30051636.
- ↑ zwonull media GbR. "cars-int.org: CARS 2013". cars-int.org. Archived from the original on 2014-03-18.