Intrauterine growth restriction (IUGR), or fetal growth restriction, is the poor growth of a fetus while in the womb during pregnancy. IUGR is defined by clinical features of malnutrition and evidence of reduced growth regardless of an infant's birth weight percentile. The causes of IUGR are broad and may involve maternal, fetal, or placental complications.

Pre-eclampsia is a multi-system disorder specific to pregnancy, characterized by the new onset of high blood pressure and often a significant amount of protein in the urine or by the new onset of high blood pressure along with significant end-organ damage, with or without the proteinuria. When it arises, the condition begins after 20 weeks of pregnancy. In severe cases of the disease there may be red blood cell breakdown, a low blood platelet count, impaired liver function, kidney dysfunction, swelling, shortness of breath due to fluid in the lungs, or visual disturbances. Pre-eclampsia increases the risk of undesirable as well as lethal outcomes for both the mother and the fetus including preterm labor. If left untreated, it may result in seizures at which point it is known as eclampsia.

Preterm birth, also known as premature birth, is the birth of a baby at fewer than 37 weeks gestational age, as opposed to full-term delivery at approximately 40 weeks. Extreme preterm is less than 28 weeks, very early preterm birth is between 28 and 32 weeks, early preterm birth occurs between 32 and 34 weeks, late preterm birth is between 34 and 36 weeks' gestation. These babies are also known as premature babies or colloquially preemies or premmies. Symptoms of preterm labor include uterine contractions which occur more often than every ten minutes and/or the leaking of fluid from the vagina before 37 weeks. Premature infants are at greater risk for cerebral palsy, delays in development, hearing problems and problems with their vision. The earlier a baby is born, the greater these risks will be.
In obstetrics, gestational age is a measure of the age of a pregnancy taken from the beginning of the woman's last menstrual period (LMP), or the corresponding age of the gestation as estimated by a more accurate method, if available. Such methods include adding 14 days to a known duration since fertilization, or by obstetric ultrasonography. The popularity of using this measure of pregnancy is largely due to convenience: menstruation is usually noticed, while there is generally no convenient way to discern when fertilization or implantation occurred.

Birth weight is the body weight of a baby at their birth. The average birth weight in babies of European and African descent is 3.5 kilograms (7.7 lb), with the normative range between 2.5 and 4.0 kilograms. On average, babies of Asian descent weigh about 3.25 kilograms (7.2 lb). The prevalence of low birth weight has changed over time. Trends show a slight decrease from 7.9% (1970) to 6.8% (1980), then a slight increase to 8.3% (2006), to the current levels of 8.2% (2016). The prevalence of low birth weights has trended slightly upward from 2012 to the present.

Complications of pregnancy are health problems that are related to, or arise during pregnancy. Complications that occur primarily during childbirth are termed obstetric labor complications, and problems that occur primarily after childbirth are termed puerperal disorders. While some complications improve or are fully resolved after pregnancy, some may lead to lasting effects, morbidity, or in the most severe cases, maternal or fetal mortality.

Intrauterine hypoxia occurs when the fetus is deprived of an adequate supply of oxygen. It may be due to a variety of reasons such as prolapse or occlusion of the umbilical cord, placental infarction, maternal diabetes and maternal smoking. Intrauterine growth restriction may cause or be the result of hypoxia. Intrauterine hypoxia can cause cellular damage that occurs within the central nervous system. This results in an increased mortality rate, including an increased risk of sudden infant death syndrome (SIDS). Oxygen deprivation in the fetus and neonate have been implicated as either a primary or as a contributing risk factor in numerous neurological and neuropsychiatric disorders such as epilepsy, attention deficit hyperactivity disorder, eating disorders and cerebral palsy.
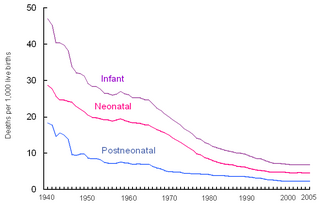
Perinatal mortality (PNM) is the death of a fetus or neonate and is the basis to calculate the perinatal mortality rate. Perinatal means "relating to the period starting a few weeks before birth and including the birth and a few weeks after birth."
Maternal obesity refers to obesity of a woman during pregnancy. Parental obesity refers to obesity of either parent during pregnancy.
The Canadian Perinatal Network (CPN) is made up of Canadian researchers who collaborate on research issues relating to perinatal care. The network commenced in September 2005, and includes members from 25 tertiary perinatal units. CPN will enable health care professionals, researchers, and administrators to participate actively in clinical, epidemiologic, health services, health policy, and informatics research aimed at improving the effectiveness and efficiency of perinatal care.

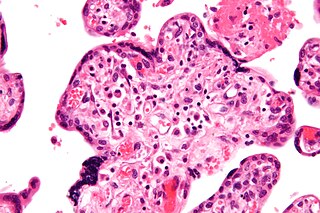
Circumvallate placenta is a rare condition affecting about 1-2% of pregnancies, in which the amnion and chorion fetal membranes essentially "double back" on the fetal side around the edges of the placenta. After delivery, a circumvallate placenta has a thick ring of membranes on its fetal surface. Circumvallate placenta is a placental morphological abnormality associated with increased fetal morbidity and mortality due to the restricted availability of nutrients and oxygen to the developing fetus.
David A. Savitz is a professor of Community Health in the Epidemiology Section of the Program in Public Health, Vice President for Research, and Professor of Obstetrics and Gynecology, at The Alpert Medical School of Brown University, and Associate Director for Perinatal Research in The Department of Obstetrics and Gynecology at Women & Infants Hospital, both in Providence, Rhode Island. Savitz is the author of Interpreting epidemiologic evidence: strategies for study design and analysis (ISBN 0-19-510840-X) and more than 275 peer-reviewed articles. He was elected to the Institute of Medicine in 2007.

A high-risk pregnancy is a pregnancy where the mother or the fetus has an increased risk of adverse outcomes compared to uncomplicated pregnancies. No concrete guidelines currently exist for distinguishing “high-risk” pregnancies from “low-risk” pregnancies; however, there are certain studied conditions that have been shown to put the mother or fetus at a higher risk of poor outcomes. These conditions can be classified into three main categories: health problems in the mother that occur before she becomes pregnant, health problems in the mother that occur during pregnancy, and certain health conditions with the fetus.
A pre-existing disease in pregnancy is a disease that is not directly caused by the pregnancy, in contrast to various complications of pregnancy, but which may become worse or be a potential risk to the pregnancy. A major component of this risk can result from necessary use of drugs in pregnancy to manage the disease.
Hypertensive disease of pregnancy, also known as maternal hypertensive disorder, is a group of high blood pressure disorders that include preeclampsia, preeclampsia superimposed on chronic hypertension, gestational hypertension, and chronic hypertension.

Caroline Anne Crowther is an Australian/New Zealand medical researcher specialising in maternity and child health. She is associated with both the University of Auckland and the University of Adelaide, being a professor at each institution. Crowther has been the recipient of multiple medical research grants.

COVID-19 infection in pregnancy is associated with several pregnancy complications. However, pregnancy does not appear to increase the susceptibility of becoming infected by COVID-19. Recommendations for the prevention of COVID-19 include the same measures as non-pregnant people.
Judith McAra-Couper is a New Zealand academic and a professor of midwifery at Auckland University of Technology.
Maternal health outcomes differ significantly between racial groups within the United States. The American College of Obstetricians and Gynecologists describes these disparities in obstetric outcomes as "prevalent and persistent." Black, indigenous, and people of color are disproportionately affected by many of the maternal health outcomes listed as national objectives in the U.S. Department of Health and Human Services's national health objectives program, Healthy People 2030. The American Public Health Association considers maternal mortality to be a human rights issue, also noting the disparate rates of Black maternal death. Race affects maternal health throughout the pregnancy continuum, beginning prior to conception and continuing through pregnancy (antepartum), during labor and childbirth (intrapartum), and after birth (postpartum).

Florence Joyce Cowan is a New Zealand midwife and educator, and an authority on pre-eclampsia. She was co-founder and director of the charity NZ Action on Pre-eclampsia, and introduced the GAP programme to monitor the growth of small babies. In 2023 Cowan was appointed an Officer of the New Zealand Order of Merit for services to midwifery, after a more than fifty year career contributing to the profession.
