Orthodontics is a dentistry specialty that addresses the diagnosis, prevention, management, and correction of mal-positioned teeth and jaws, as well as misaligned bite patterns. It may also address the modification of facial growth, known as dentofacial orthopedics.

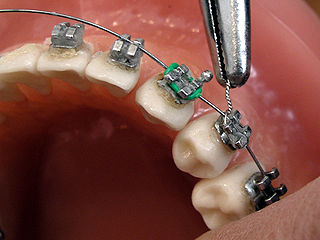
Dental braces are devices used in orthodontics that align and straighten teeth and help position them with regard to a person's bite, while also aiming to improve dental health. They are often used to correct underbites, as well as malocclusions, overbites, open bites, gaps, deep bites, cross bites, crooked teeth, and various other flaws of the teeth and jaw. Braces can be either cosmetic or structural. Dental braces are often used in conjunction with other orthodontic appliances to help widen the palate or jaws and to otherwise assist in shaping the teeth and jaws.

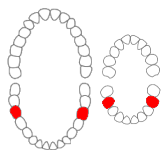
The premolars, also called premolar teeth, or bicuspids, are transitional teeth located between the canine and molar teeth. In humans, there are two premolars per quadrant in the permanent set of teeth, making eight premolars total in the mouth. They have at least two cusps. Premolars can be considered transitional teeth during chewing, or mastication. They have properties of both the canines, that lie anterior and molars that lie posterior, and so food can be transferred from the canines to the premolars and finally to the molars for grinding, instead of directly from the canines to the molars.
Hypodontia is defined as the developmental absence of one or more teeth excluding the third molars. It is one of the most common dental anomalies, and can have a negative impact on function, and also appearance. It rarely occurs in primary teeth and the most commonly affected are the adult second premolars and the upper lateral incisors. It usually occurs as part of a syndrome that involves other abnormalities and requires multidisciplinary treatment.

In orthodontics, a malocclusion is a misalignment or incorrect relation between the teeth of the upper and lower dental arches when they approach each other as the jaws close. The English-language term dates from 1864; Edward Angle (1855-1930), the "father of modern orthodontics", popularised it. The word "malocclusion" derives from occlusion, and refers to the manner in which opposing teeth meet.

A palatal expander is a device in the field of orthodontics which is used to widen the upper jaw (maxilla) so that the bottom and upper teeth will fit together better. This is a common orthodontic procedure. The use of an expander is most common in children and adolescents 8–18 years of age. It can also be used in adults, although expansion is more uncomfortable and takes longer in adults. A patient who would rather not wait several months for the end result achieved by a palatal expander may be able to opt for a surgical separation of the maxilla. Use of a palatal expander is most often followed by braces to then straighten the teeth.
The mandibular first molar or six-year molar is the tooth located distally from both the mandibular second premolars of the mouth but mesial from both mandibular second molars. It is located on the mandibular (lower) arch of the mouth, and generally opposes the maxillary (upper) first molars and the maxillary 2nd premolar in normal class I occlusion. The function of this molar is similar to that of all molars in regard to grinding being the principal action during mastication, commonly known as chewing. There are usually five well-developed cusps on mandibular first molars: two on the buccal, two lingual, and one distal. The shape of the developmental and supplementary grooves, on the occlusal surface, are described as being M-shaped. There are great differences between the deciduous (baby) mandibular molars and those of the permanent mandibular molars, even though their function are similar. The permanent mandibular molars are not considered to have any teeth that precede it. Despite being named molars, the deciduous molars are followed by permanent premolars.
Dental anatomy is a field of anatomy dedicated to the study of human tooth structures. The development, appearance, and classification of teeth fall within its purview. Tooth formation begins before birth, and the teeth's eventual morphology is dictated during this time. Dental anatomy is also a taxonomical science: it is concerned with the naming of teeth and the structures of which they are made, this information serving a practical purpose in dental treatment.

Crossbite is a form of malocclusion where a tooth has a more buccal or lingual position than its corresponding antagonist tooth in the upper or lower dental arch. In other words, crossbite is a lateral misalignment of the dental arches.

An impacted tooth is one that fails to erupt into the dental arch within the expected developmental window. Because impacted teeth do not erupt, they are retained throughout the individual's lifetime unless extracted or exposed surgically. Teeth may become impacted because of adjacent teeth, dense overlying bone, excessive soft tissue or a genetic abnormality. Most often, the cause of impaction is inadequate arch length and space in which to erupt. That is the total length of the alveolar arch is smaller than the tooth arch. The wisdom teeth are frequently impacted because they are the last teeth to erupt in the oral cavity. Mandibular third molars are more commonly impacted than their maxillary counterparts.
Serial extraction is the planned extraction of certain deciduous teeth and specific permanent teeth in an orderly sequence and predetermined pattern to guide the erupting permanent teeth into a more favorable position.
Lingual braces are one of the many types of the fixed orthodontic treatment appliances available to patients needing orthodontics. They involve attaching the orthodontic brackets on the inner sides of the teeth. The main advantage of lingual braces is their near invisibility compared to the standard braces, which are attached on the buccal (cheek) sides of the tooth. Lingual braces were invented by Craven Kurz in 1976.

Anchorage in orthodontics is defined as a way of resisting movement of a tooth or number of teeth by using different techniques. Anchorage is an important consideration in the field of orthodontics as this is a concept that is used frequently when correcting malocclusions. Unplanned or unwanted tooth movement can have dire consequences in a treatment plan, and therefore using anchorage stop a certain tooth movement becomes important. Anchorage can be used from many different sources such as teeth, bone, implants or extra-orally.
Frankel appliance or Frankel Functional Regulator is an orthodontic functional appliance which was developed by Rolf Fränkel in 1950s for treatment to patients of all ages. This appliance primarily focused on the modulation of neuromuscular activity in order to produce changes in jaw and teeth. The appliance was opposite to the Bionator appliance and Activator appliance.
Molar distalization is a process in the field of Orthodontics which is used to move molar teeth, especially permanent first molars, distally (backwards) in an arch. This procedure is often used in treatment of patients who have Class 2 malocclusion. The cause is often the result of loss of E space in an arch due to early loss of primary molar teeth and mesial (forward) migration of the molar teeth. Sometimes molars are distalized to make space for other impacted teeth, such as premolars or canines, in the mouth.
ACCO or Acrylic Cervical Occipital Anchorage is an appliance in field of orthodontics which is used for distalization of maxillary molars. This appliance is a removable type of appliance which was developed by Herbert I. Margolis. This appliance is intended to be worn 24 hours a day except during meals. It is one of the few removable appliances made for distalization of molars and thus require patient compliance for the treatment to be successful.
Intrusion is a movement in the field of orthodontics where a tooth is moved partially into the bone. Intrusion is done in orthodontics to correct an anterior deep bite or in some cases intrusion of the over-erupted posterior teeth with no opposing tooth. Intrusion can be done in many ways and consists of many different types. Intrusion, in orthodontic history, was initially defined as problematic in early 1900s and was known to cause periodontal effects such as root resorption and recession. However, in mid 1950s successful intrusion with light continuous forces was demonstrated. Charles J. Burstone defined intrusion to be "the apical movement of the geometric center of the root (centroid) in respect to the occlusal plane or plane based on the long axis of tooth".
An ectopic maxillary canine is a canine which is following abnormal path of eruption in the maxilla. An impacted tooth is one which is blocked from erupting by a physical barrier in the path of eruption. Ectopic eruption may lead to impaction. Previously, it was assumed that 85% of ectopic canines are displaced palatally, however a recent study suggests the true occurrence is closer to 50%. While maxillary canines can also be displaced buccally, it is thought this arises as a result of a lack of space. Most of these cases resolve themselves with the permanent canine erupting without intervention.
Orthodontic indices are one of the tools that are available for orthodontists to grade and assess malocclusion. Orthodontic indices can be useful for an epidemiologist to analyse prevalence and severity of malocclusion in any population.

